
Download
Original Research
Hepatic glycogenosis in glycogenic hepatopathy and Metabolic dysfunction associated fatty liver disease
Monica Chandrasekar1, Sakthisankari Shanmugasundaram1,*
1Department of Pathology, PSG Institute of Medical Sciences and Research, 641004 Coimbatore, India
Abstract
Background: Glycogenic hepatopathy (GH) is a rare complication of uncontrolled type 1 diabetes mellitus (T1DM) in children and was originally described as Mauriac syndrome. Identified as a prominent glycogenosis of hepatocytes, it has also been reported in adults in other conditions, including type 2 diabetes mellitus (T2DM). It clinically mimics Metabolic dysfunction associated fatty liver disease (MAFLD). The study describes five cases of glycogenic hepatopathy and compares the clinicopathological findings with that of MAFLD. Methods: Cases with hepatic parenchymal glycogenosis diagnosed during the study period were included. These cases were grouped into glycogenic hepatopathy and MAFLD based on their histological features and corresponded with their transaminase levels. Results: Out of 261 liver biopsies received during the study period (3 years), 16 cases with parenchymal glycogenosis were included in the study. Cases with pale, rarefied, enlarged hepatocytes (periodic acid Schiff-positive, diastase sensitive) with prominent plasma membranes with diffuse glycogenosis were diagnosed as GH (Group 1). Five cases of GH were identified, all females, associated with T2DM (n = 3), hypothyroidism (n = 1) and elevated liver enzymes (n = 5). Normalization of enzymes after glycemic control was seen in n = 3/5 cases. The remaining 11 cases (Group 2) showed hepatic steatosis, focal hepatic glycogenosis & fibrosis with persistent elevation of liver enzymes following treatment. Conclusions: All cases of glycogenic hepatopathy in this study were females and none of them were associated with type 1 diabetes mellitus, which is implicated as the most common underlying etiology worldwide. This study suggests that glycogenic hepatopathy may be more common in adults with T2DM or other metabolic derangements than anticipated and have a female preponderance.
Keywords: Glycogenic hepatopathy; Hepatic parenchymal glycogenosis; Metabolic dysfunction associated fatty liver disease
Submitted: 23 January 2025; Accepted: 13 May 2025; Published: 20 June 2026
Authors for correspondence: Emails: sakthissankari@gmail.com
How to cite: Monica Chandrasekar, Sakthisankari Shanmugasundaram. Hepatic glycogenosis in glycogenic hepatopathy and metabolic dysfunction associated fatty liver disease. Journal of Renal and Hepatic Disorders. 2026; 10(1): 34-40. doi: 10.63268/jrenhp.v10i1.216.
DOI: 10.63268/jrenhp.v10i1.216
Copyright: The Author(s). Published by Troika Publisher. License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
The liver, being the key regulator of carbohydrate metabolism, can be affected by dysregulation in glycogen metabolism, which occurs in systemic conditions [1]. These conditions include glycogen storage disorders, diabetes mellitus and Metabolic Dysfunction Associated Fatty Liver Disease (MAFLD), and can result in hepatic dysfunction presenting as transaminitis [2]. The light microscopic examination demonstrates increased parenchymal glycogenosis [3]. The normal hepatocytes contain glycogen which is not demonstrable in hematoxylin and eosin-stained sections. Periodic acid Schiff stain (PAS) stains the glycogen magenta and since glycogen is digestible by amylase (diastase), subsequent treatment with diastase dissolves the glycogen present in the hepatocytes. In the setting of excess glycogen in the liver, it can be appreciated in routine Hematoxylin & eosin stain (H&E) as enlarged hepatocytes with pale, rarefied cytoplasm (PAS positive and diastase-sensitive) & prominent plasma membranes [3, 4].
One such cause for excessive parenchymal glycogenosis is Mauriac syndrome described by Pierre Mauriac in a pediatric patient with poorly controlled type 1 diabetes mellitus (T1DM) [3]. Since then, various terminologies like hepatic glycogen storage, hepatic glycogenosis, glycogenic hepatopathy (GH) and glycogen storage hepatomegaly have been used to describe this entity [5]. GH is clinically characterized by the transient elevation of liver enzymes with hepatomegaly and reversible glycogenosis of liver parenchyma. GH is rarely reported in type 2 diabetes mellitus (T2DM) [6] and other conditions like anorexia nervosa, dumping syndrome, high-dose glucocorticoid therapy and hypothyroidism [5]. Focal or diffuse hepatic glycogenesis has been reported to be associated with or precede the development of hepatocellular carcinoma (HCC) as observed in various animal models of carcinogenesis and in patients with chronic liver disease prone to develop HCC. The term focal hepatic preneoplasia has been used to describe these entities [7].
The other causes for hepatic parenchymal glycogenosis include MAFLD, urea cycle defects, glycogen storage disorders and drug-induced pseudo ground glass inclusions in hepatocytes [4, 5]. There are many case reports describing the occurrence of GH in T1DM patients. Even though rare, GH in the absence of T1DM is being reported [6, 8]. The present study aims to assess the clinicopathological profile and the role of liver biopsy in patients with hepatic parenchymal glycogenosis.
Materials and methods
Cases with hepatic parenchymal glycogenosis over 3 years from January 2020 to December 2022 were retrospectively reviewed after obtaining institutional human ethics committee approval. Group 1comprised cases with diffuse parenchymal glycogenosis of more than 50%. Cases of steatosis and/or fibrosis with focal parenchymal glycogenosis occurring in patients with DM, obesity or metabolic syndrome (Metabolic Dysfunction Associated Fatty Liver Disease) were included under Group 2.
Glycogen storage disorders and other specific etiologies like Wilson’s disease were excluded from the study. Relevant clinical, laboratory and imaging data of these patients were collected. The values of liver enzymes, including alanine transaminase (ALT) and aspartate transaminase (AST) before and after treatment, were also collected. The liver biopsies were routinely fixed in 10% neutral buffered formalin and paraffin embedded. 5-micron sections were cut and stained with H&E. H&E stained sections, along with Masson trichrome stain (MTS), Reticulin stain and Periodic acid-Schiff (PAS) and PAS with diastase (PAS-D) stains, were reviewed. PAS stain was used to demonstrate the glycogenosis, further enhanced by diastase digestion. There were no specific processing and staining techniques followed in the current study. The biopsies were evaluated by two pathologists individually for the following details. A consensus regarding the scoring of fibrosis and steatosis was obtained before evaluation.
• Presence of glycogenosis;
• Glycogenated nuclei;
• Steatosis (Grade I: <5%, II: 6–33%, III: 34 to 66% and IV: >66%);
• Metavir Scoring for Fibrosis (F1 to F4, portal fibrosis without septa, portal fibrosis with septa formation, bridging fibrosis and cirrhosis, respectively).
Cases with pale, rarefied, enlarged hepatocytes with prominent plasma membranes (PAS positive & Diastase sensitive) were categorized as glycogenic hepatopathy. The histological features of the two groups were analyzed and compared with etiology and serum transaminase levels.
Results
There were 261 liver biopsies received during the study period. 16 cases that met the inclusion criteria were included in the study. There were 5 cases in the glycogenic hepatopathy category (Group 1). The remaining 11 were categorized under the steatotic group with focal glycogenosis (Group 2).
Glycogenic hepatopathy
The clinical manifestation included persistent transaminitis in 80% of cases. All five cases were females with a mean age group of 59 years (n = 4 cases). There was one child aged 11 years. Among the five cases, three were type 2 diabetics, and one was a case of hypothyroidism. The three patients were on oral hypoglycemics and not on insulin. Serum transaminases (ALT & AST) were elevated 2 to 5 times the normal range in 80% (n = 4/5) of cases. Abdominal distension and discomfort were reported in 60% (n = 3/5) of cases. Elevation of alkaline phosphatase was observed in 60% of cases (n = 3/5) and Glycated hemoglobin A (HbA1c) in 20% of cases (n = 1/5). Serological markers for viruses were negative in all the cases. Autoimmune work up turned out positive in 60% (n = 3/5) of cases (liver IgG (Immunoglobulin gamma), Anti-soluble liver antigen/liver-pancreas (SLA/LP) (n = 1); Antinuclear antibody (ANA), Antibodies to Ro52 + (n = 1); cytoplasmic-Antineutrophil cytoplasmic antibody (ANCA-c) + (n = 1)).
Computed Tomography (CT) (n = 3) and Magnetic Resonance Imaging (MRI) (n = 1) showed features of chronic parenchymal liver disease in 3 cases and mild to moderate fatty infiltration in 1 case. Ultrasound imaging revealed normal liver parenchyma in 1 case. The demographic, clinical, biochemical, and radiographic findings of the GH group are listed in Table 1.
Table 1: Summary of the demographic, clinical, biochemical and radiographic findings of all cases.
| No. | Parameters | Group 1 Glycogenic hepatopathy n = 5 |
Group 2 Metabolic dysfunction associated fatty liver disease n = 11 | |
| 1 | Age | ≤40 yr | 1/5 (20%) | 3/11 (18.1%) |
| 40–60 yr | 1/5 (20%) | 8/11 (72.7%) | ||
| >60 yr | 3/5 (60%) | - | ||
| 2 | Sex | Female | 5/5 (100%) | 8/11 (72.7%) |
| Male | 0/5 | 3/11 (27.3%) | ||
| 3 | Etiology/Comorbidities | Type 2 Diabetes mellitus | 3/5 (60%) | 7/11 (63.6%) |
| Hypothyroidism | 1/5 (20%) | 4/11 (36.3%) | ||
| No known comorbidities | 1/5 (20%) | - | ||
| 4 | Clinical presentation | Persistent transaminitis (elevated ALT, AST) | 4/5 (80%) | 7/11 (63.6%) |
| Abdominal distension/discomfort | 3/5 (60%) | 4/11 (36.3%) | ||
| 5 | Imaging (MRI/CT/USG) | Fatty liver | 1/5 (20%) | 9/11 (81.8%) |
| Chronic parenchymal liver disease | 3/5 (60%) | 2/11 (18.2%) | ||
| Normal | 1/5 (20%) | - | ||
| 6 | AST/ALT on follow up | Normal/Reduced | 3/5 (60%) | 3/11 (27.3%) |
| Persistent elevation | 1/5 (20%) | 9/11 (81.8%) | ||
| Lost to follow up | 1/5 (20%) | - | ||
ALT: alanine transaminase; AST: aspartate transaminase; MRI: Magnetic Resonance Imaging; CT: Computed tomography; USG: Ultrasonography.
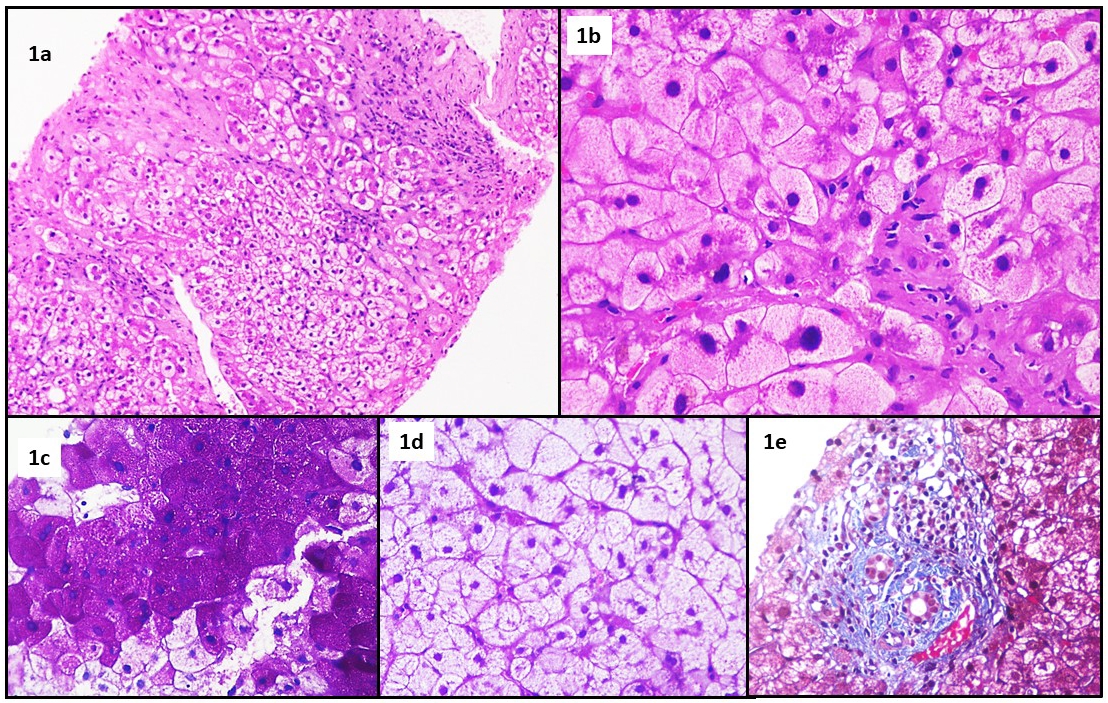
On histopathological examination, all five cases showed diffuse PAS positive, diastase sensitive pale rarefied enlarged hepatocytes (Fig. 1a–d). Focal steatosis was observed in 40% (n = 2/5) of cases (<5%). Mild portal inflammation was observed in 40% (n = 2/5) of cases. Fibrosis (bridging fibrosis) was seen in 20% (n = 1/5) of cases (Fig. 1e).
Figure 1 A Case of glycogenic hepatopathy. (a) Low power (H&E, 10×) view of trucut biopsy of liver, showing lobular disarray with sinusoidal compression. There is extensive glycogenosis of hepatocytes which are enlarged with, pale, rarefied cytoplasm. The portal areas show minimal inflammatory infiltrate and mild fibrosis. There is no evidence of steatosis or steatohepatitis (H&E, 10×). (b) “Glycogenosis of hepatocytes”—Individual hepatocytes appear enlarged, with distinct cell borders& pale, rarefied cytoplasm imparting a plant cell-like appearance as a result of glycogen accumulation in the cytoplasm. There is marked sinusoidal compression by the enlarged hepatocytes (H&E, 40×). (c) The intracellular glycogen in the enlarged hepatocytes shows intense positivity for Periodic Acid Schiff stain (PAS, 40×). (d) These larger hepatocytes appear clear when Periodic Acid Schiff and diastase (PAS-D) are coupled, suggesting the presence of glycogen that the diastase enzyme has broken down (PAS-D, 40×). (e) The minimal fibrosis present in the portal area is highlighted by Masson’s Tricrome stain (MTS, 40×).
On follow-up after one year, the transaminase levels after good glycemic control reverted to normal in 60% (n = 3/5) cases. Of the remaining two cases, one was hypothyroid, and the other was lost to follow-up to pursue treatment in a higher centre (Table 1).
Steatotic group
Among the 11 cases, 27.3% (n = 3/11) were males, and 72.7% (n = 8/11) were females. The mean age was 46.7 years. Among these, 7 cases had underlying T2DM (with morbid obesity = 3; hypothyroidism = 2), and 4 had hypothyroidism (1 with nephrotic syndrome). Serum transaminase levels were elevated in 63.6% of cases (n = 7/11). Elevation of alkaline phosphatase was observed in 100% of cases & HbA1c in 36.3% (n = 4/11) of cases. Serology for viral markers was negative in 100% of cases. Autoimmune workup was positive in 18.1% (n = 2/11) of cases (Ro52, IgG in one case and Liver Kidney Microsomal antibody and Anti-liver cytosolic antigen type 1 (LC1) antibodies in the other case).
Ultrasound/CT showed fatty infiltration of liver parenchyma (ranging from mild to severe) with features of chronic parenchymal liver disease in all cases. The demographic, clinical, biochemical and radiographic findings of the steatotic group are summarized in Table 1.
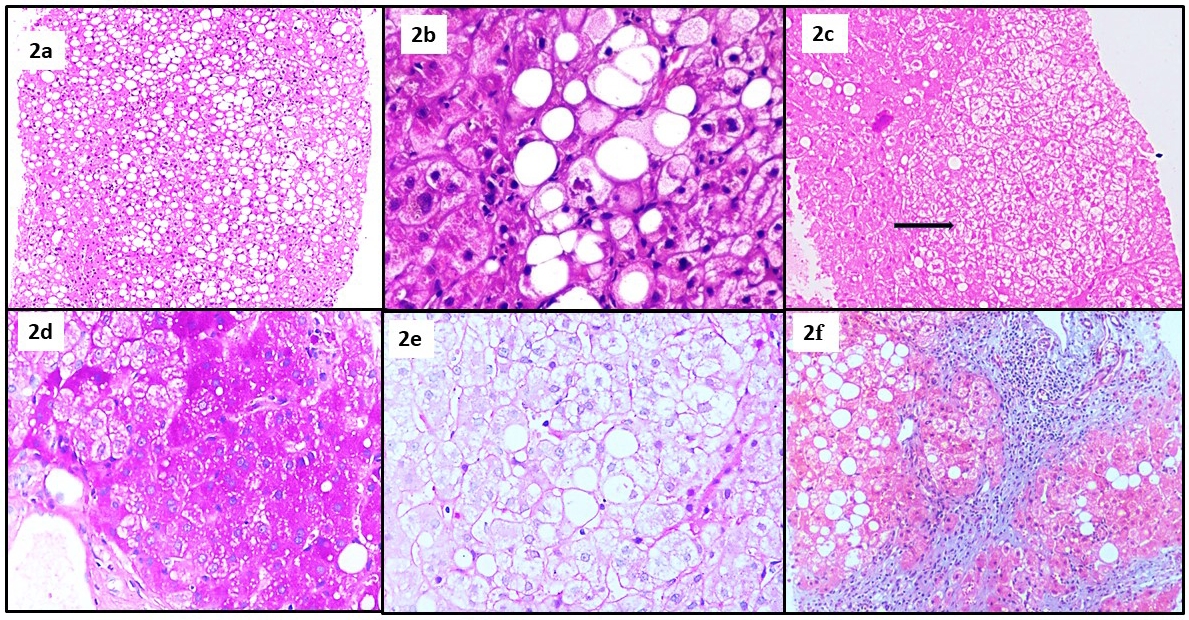
Histopathological examination revealed a macrovesicular type of steatosis (steatosis <33% in 4 cases; 34 to 64% in 6 cases; >65% in 1 case) (Fig. 2a,b) and focal parenchymal glycogenosis in all the cases (Fig. 2c–e). Mild portal inflammation was present in 63.6% of cases. Portal fibrosis was observed in 90% of cases (bridging fibrosis in 2 cases and septal fibrosis in 3 cases) (Fig. 2f).
Figure 2 A case of MAFLD. (a) Low power view of liver parenchyma showing lobular disarray, diffuse macrovesicular steatosis and lobular inflammation (H&E; 10×). (b) Hepatocytes show intracytoplasmic clear fat vacoules with a peripherally pushed nucleus (macrovesicular steatosis) and are accompanied by surrounding inflammatory cells (H&E, 40×). (c) Focal hepatocyte glycogenosis (intracellular glycogen accumulation) in a case of MAFLD, as marked by enlarged hepatocytes with pale rarefied cytoplasm (black arrow) (H&E, 10×). (d,e) These enlarged hepatocytes with pale rarefied cytoplasm show intense positivity with PAS stain (d) which when coupled with diastase (PAS-D) shows clear cytoplasm (e) indicating the presence of glycogen. (f) Masson’s trichrome stain (MTS) highlights marked periportal and septal fibrosis. The portal area also shows a dense portal inflammation (MTS, 40×).
While parenchymal glycogenosis (diffuse or focal) was observed in both groups, tangible difference was noted between the two groups with regard to other histopathological features summarized in Table 2.
Table 2: Histopathological findings in GH and MAFLD.
| No | Parameters | Group 1 Glycogenic hepatopathy n = 5 |
Group 2 MAFLD n = 11 | |
| 1 | Steatosis | <5% | 2 (40%) | 0 |
| 5–33% | 0 | 4 (36.3%) | ||
| 34–66% | 0 | 6 (54.5%) | ||
| >66% | 0 | 1 (9.1%) | ||
| 2 | Fibrosis | F1 | 0 | 5 (45.4%) |
| F2 | 0 | 3 (27.2%) | ||
| F3 | 1 (20%) | 2 (18.1%) | ||
| F4 | 0 | 0 | ||
| 3 | Portal inflammation | Mild | 2 (40%) | 7 (63.6%) |
| Moderate | 0 | 2 (18.1%) | ||
MAFLD: Metabolic dysfunction associated fatty liver disease.
Discussion
The study was conducted to understand the role of histopathology in differentiating glycogenic hepatopathy from the parenchymal glycogenosis in MAFLD. The most common cause of hepatomegaly with transaminitis in diabetes is MAFLD followed by Glycogenic hepatopathy. GH mimics MAFLD clinically [9]. Patients present with abdominal discomfort, distension and elevated liver enzymes with evidence of parenchymal liver disease on radiography [3]. Various factors help in distinguishing the two conditions, liver biopsy being the most crucial among them [10].
The exact incidence of GH in diabetics is largely unknown. 80% of cases of GH in our study had T2DM, in contrast to the 98% of GH cases reported in T1DM. Glycogenic hepatopathy has been reported in children or young adults with type 1 diabetes or other etiologies [11]. Uncontrolled blood glucose levels have been found to play a role in the pathogenesis, as evidenced by prior recurrent episodes of diabetic ketoacidosis (DKA) and elevated HbA1clevels in these patients [12]. The insulin-independent, passive diffusion of glucose into the hepatocytes during episodes of hyperglycemia and its subsequent conversion into glycogen, under the influence of insulin, has been hypothesized to result in excessive parenchymal glycogen accumulation in cases of T1DM [13]. The underlying insulin resistance in T2DM causes decreased glycogen synthesis, however, rare instances of GH have been reported in T2DM [6]. The reason for this paradoxical glycogen accumulation in DM is unknown. Tsujimoto et al. [14] reported a case of rapid onset of hepatomegaly with altered liver enzymes due to glycogen accumulation in a 41-year-old male with T2DM, who self-administered an excessive dose of long-acting insulin leading to hypoglycemia and was subsequently treated with intravenous glucose injections and hypercaloric infusion [14]. A special case report by Umpaichitra et al. [15], on a 15-year-old morbidly obese male with no prior evidence of T1DM presented with altered liver function tests, hepatomegaly, high HbA1c levels, and the liver biopsy showing diffuse excessive parenchymal glycogenosis, was diagnosed as T2DM and started on metformin [15]. His follow-up liver biopsy showed a reversal of glycogenosis with normal liver architecture.
Apart from DM, its occurrence has been reported in various other conditions like hypothyroidism, anorexia nervosa, dumping syndrome, long-term steroid therapy and focal hepatic preneoplasia [2, 3, 10]. Altered glucose metabolism in these conditions is thought to precipitate glycogenosis. 20% of our cases with GH (n = 1/5) had a prior history of hypothyroidism.
A slight female predominance of 77% has been reported in GH [5]. While the association between MAFLD and the female gender has been well established, fewer reports are available indicating its association with glycogenic hepatopathy. All the cases encountered in this study are females.
The clinical presentation of GH can vary from asymptomatic transaminitis with hepatomegaly to symptoms of ketoacidosis with hyperglycemia [9]. Abdominal pain and hepatomegaly were the most common presenting features in various reports [10, 12]. Rapid enlargement of the liver due to glycogen accumulation causes stretching of the capsule, causing abdominal pain [16]. 60% (n = 3) of GH cases in this study presented with gradual abdominal distension with pain and bilateral pedal edema, while the remaining 40% had persistent asymptomatic transaminitis. The glycogen-laden enlarged hepatocytes can cause sinusoidal compression, leading to ascites in rare cases [9]. One such case in this study presented mild ascites.
Most reported cases have elevated aspartate and aminotransferase levels, while the elevation of alkaline phosphatase levels was rare [5]. There is usually no alteration of synthetic functions of the liver. The histologic features have not, in the past, favored necrosis as the cause for enzyme elevation but have rather been attributed to the leakage of enzymes from hepatocytes with glycogen accumulation [17]. In the study conducted by Mukewar et al. [3], transaminase levels were markedly elevated (even up to 10 times) in T1DM cases with GH than in those T1DM cases without GH. In our study, the serum transaminases (ALT & AST) were elevated 2 to 5 times the normal range in 60% (n = 3) of GH cases. Elevation of alkaline phosphatase was observed in 60% of GH cases (n = 3). Normalization of transaminase levels following treatment was significant in the GH group compared to the MAFLD group. Recurrent episodes of diabetic ketoacidosis (DKA) and elevated HbA1c levels have been reported commonly in GH. The reported mean Hemoglobin A1c in cases of GH is 11.8 g/dL [12]. Although there was no evidence of prior DKA in these patients, the mild elevation in HbA1c levels in some of them, together with an underlying metabolic abnormality, implies deranged glucose levels in these subjects over a while. Radiological features usually point toward a parenchymal disease with increased parenchymal echogenicity [4]. The radiological findings in this study included features suggesting a chronic parenchymal liver disease (n = 3/5) or fatty liver (n = 1/5).
While the clinical, laboratory and radiological findings are found to be overlapping in MAFLD and GH, it is the liver biopsy findings that clinch the diagnosis of GH [9]. The rationale behind differentiating is that while MAFLD has the potential for progressive liver fibrosis and cirrhosis, GH is reversible, with good glycemic control being the mainstay of treatment [8].
The causes for hepatomegaly in diabetes are glycogen accumulation and a fatty liver. In contrast to MAFLD, the steatosis was minimal in GH, while the stage of fibrosis varied. Torbenson et al. [13], demonstrated minimal steatosis in 14% (2/14) of cases, with mild steatohepatitis in 7% (1/14) and mild fibrosis in 14% (2/14) of cases. Fibrosis is not a typical feature of GH. Untreated cases of glycogenic hepatopathy can progress to fibrosis and cirrhosis without steatosis. Fibrosis is not a typical feature of GH [18]. In our series, a single case showed bridging fibrosis. Similarly, steatosis & inflammation are rarely reported. However, Fitzpatrick et al. [17] reported inflammation, steatosis and fibrosis in cases of GH. So far, three cases have been reported to be associated with significant fibrosis. The exact mechanism leading to the development of fibrosis in GH is unclear. Fibrosis is a component ofmetabolic dysfunction associated steatohepatitis. Diabetic microangiopathy affecting the liver can result in significant fibrosis which is called diabetic hepatosclerosis. The fibrosis in hepatosclerosis is usually perisinusoidal [4]. The long-term effects of fibrosis in GH are unknown. These individuals might have significant fibrosis in adulthood [5]. It is essential to differentiate fibrosis and diabetic hepatosclerosis in GH.
Cases of MAFLD can display excess glycogenosis of hepatocytes. These changes have been typically described in T2DM and other metabolic syndromes. Glycogenated hepatocytes have been reported in 54% of MAFLD cases [9]. Glycogenosis is common in nonalcoholic fatty liver disease and is independently associated with ballooning but lower steatosis and lower fibrosis [9]. However, as discussed by Ribback et al. [16], observations in various animal models of hepatocarcinogenesis and type 2 diabetes suggest that the dysfunction of glucose metabolism resulting in the combination of glycogenosis and steatosis, or steatosis alone, in ballooned hepatocytes is a secondary rather than primary metabolic change appearing predominantly during progression.
The glycogenated hepatocytes observed in MAFLD showed a similar morphology as that of the glycogenic hepatopathy. However, these changes are patchy, not diffuse and predominantly centrilobular [3]. These changes can be misinterpreted as ballooned hepatocytes in cases of MAFLD. PAS and PAS-D stains help in ascertaining the nature of these hepatocytes [2]. Cases of MAFLD with glycogenosis are reported to be associated with decreased steatosis [4]. However, we did not find any such association in the current study. None of the cases were associated with hepatocellular carcinoma in the present study. Bannasch et al. [7] in their study, had described a possible link between hepatic glycogenosis and hepatocellular carcinoma.
Liver biopsy can differentiate the two clinically, biochemically and radiologically overlapping entities, GH and MAFLD [5]. Though the progression to advanced fibrosis and cirrhosis without steatosis or steatohepatitis varies among cases, the fact that complete reversal can be achieved through early identification and treatment calls for a thorough evaluation in suspected cases, where liver biopsy has a vital role.
Limitations
The authors acknowledge the limitations of the study: (1) Small sample size and hence statistical analysis could not be performed and the results cannot be generalized. (2) Non-availability of follow-up liver biopsies to demonstrate the reversal of parenchymal glycogenosis. (3) No specific processing techniques to prevent the elution of glycogen from hepatocytes were performed in the current study that could have resulted in the regional variation of hepatic glycogenosis within the slides. (4) Retrospective nature of the study. Given the rarity of the disease per se and the observation of fibrosis in glycogen hepatopathy, longitudinal follow-up is essential for a better understanding of the outcome of glycogenic hepatopathy.
Conclusions
The present findings, similar to other studies into this relatively newer entity, suggest that glycogenic hepatopathy is not exclusive to children with type 1 diabetes mellitus but also in adults with type 2 diabetes mellitus or other metabolic conditions and might have a female predominance. Further insight into the incidence, prevalence and distribution pattern concerning the underlying etiology is required to diagnose this potentially reversible liver disease accurately.
Availability of data and materials
The data are contained within this article.
Author contributions
MC—designed the research study, analysed the data and wrote the manuscript. SS—conceptualized the study, analysed the data and wrote the manuscript. Both authors contributed to the editorial changes in the manuscript. Both authors read and approved the final manuscript.
Ethics approval and consent to participate
The study received ethics approval from the PSGIMSR Institutional Human Ethics Committee (approval number: PSG/IHEC/2023/Appr/Exp/364), and informed consent was obtained from all participants.
Acknowledgment
We thank Nirmala V, for her contribution to the scoring and reporting of the cases and the Departments of Gastroenterology and Radiology for their invaluable contribution towards this research.
Funding
This research received no external funding.
Conflict of interest
The authors declare no conflict of interest.
REFERENCES
1. Rui L. Energy metabolism in the liver. Comprehensive Physiology. 2014; 4: 177–197.
2. Soon GST, Torbenson M. The liver and glycogen: in sickness and in health. International Journal of Molecular Sciences. 2023; 24: 6133.
3. Mukewar S, Sharma A, Lackore KA, Enders FT, Torbenson MS, Kamath PS, et al. Clinical, biochemical, and histopathology features of patients with glycogenic hepatopathy. Clinical Gastroenterology and Hepatology. 2017; 15: 927–933.
4. Kshirsagar RK, Sharman T. Glycogenic hepatopathy. StatPearls Publishing: Treasure Island (FL). 2025.
5. Sherigar JM, Castro JD, Yin YM, Guss D, Mohanty SR. Glycogenic hepatopathy: a narrative review. World Journal of Hepatology. 2018; 10: 172–185.
6. Cox BK, Guindi M, Hutchings D, Kim SA, Waters KM, Larson BK. Glycogenic hepatopathy is associated with type 1 diabetes mellitus in only a minority of cases in a contemporary adult population. Annals of Diagnostic Pathology. 2023; 64: 152130.
7. Bannasch P, Ribback S, Su Q, Mayer D. Clear cell hepatocellular carcinoma: origin, metabolic traits and fate of glycogenotic clear and ground glass cells. Hepatobiliary & Pancreatic Diseases International. 2017; 16: 570–594.
8. Garcês Soares S, Medas R, Conceição F, Silva R, Paiva JA, Carneiro AC. Hepatic glycogenosis: an underdiagnosed entity? Cureus. 2022; 14: e23853.
9. Allende DS, Gawrieh S, Cummings OW, Belt P, Wilson L, Van Natta M, et al. Glycogenosis is common in nonalcoholic fatty liver disease and is independently associated with ballooning, but lower steatosis and lower fibrosis. Liver International. 2021; 41: 996–1011.
10. Parmar N, Atiq M, Austin L, Miller RA, Smyrk T, Ahmed K. Glycogenic hepatopathy: thinking outside the box. Case Reports in Gastroenterology. 2015; 9: 221–226.
11. Sjöholm Å, Mahma H. Glycogenic hepatopathy. The New England Journal of Medicine. 2024; 391: 1528.
12. Aluko A, Enofe I, Burch J, Yam J, Khan N. Hepatocellular glycogen accumulation in the setting of poorly controlled type 1 diabetes mellitus: case report and review of the literature. Case Reports in Hepatology. 2020; 2020: 9368348.
13. Torbenson M, Chen YY, Brunt E, Cummings OW, Gottfried M, Jakate S, et al. Glycogenic hepatopathy: an underrecognized hepatic complication of diabetes mellitus. The American Journal of Surgical Pathology. 2006; 30: 508–513.
14. Tsujimoto T, Takano M, Nishiofuku M, Yoshiji H, Matsumura Y, Kuriyama S, et al. Rapid onset of glycogen storage hepatomegaly in a type-2 diabetic patient after a massive dose of long-acting insulin and large doses of glucose. Internal Medicine. 2006; 45: 469–473.
15. Umpaichitra V. Unusual glycogenic hepatopathy causing abnormal liver enzymes in a morbidly obese adolescent with well-controlled type 2 diabetes: resolved after A1c was normalized by metformin. Clinical Obesity. 2016; 6: 281–284.
16. Ribback S, Peters K, Yasser M, Prey J, Wilhelmi P, Su Q, et al. Hepatocellular ballooning is due to highly pronounced glycogenosis potentially associated with steatosis and metabolic reprogramming. Journal of Clinical and Translational Hepatology. 2024; 12: 52–61.
17. Fitzpatrick E, Cotoi C, Quaglia A, Sakellariou S, Ford-Adams ME, Hadzic N. Hepatopathy of Mauriac syndrome: a retrospective review from a tertiary liver centre. Archives of Disease in Childhood. 2014; 99: 354–357.
18. Sherigar JM, Darouichi Y, Guss D, Mohanty SR. An unusual presentation of glycogenic hepatopathy with bridging fibrosis. ACG Case Reports Journal. 2018; 5: e31.