
Download
Original Research
Depression in prevalent maintenance hemodialysis patients
Jawad Iqbal Rather1,*, Amir Farooq2, Muzamil Ahmad Wani2, Nuha Saleem2,
Zeeza Hussain Shah3, Muzafar Maqsood Wani2, Imtiyaz Ahmad Wani2, Imran Khan2
1Department of Medicine, Government Medical College Anantnag, 192101 Anantnag, India
2Department of Nephrology, Sher-I Kashmir Institute of Medical Sciences, 190011 Srinagar, India
3Department of Medicine, Sher-I-Kashmir Institute of Medical Sciences, 190011 Srinagar, India
Abstract
Background: Depression is a common mental health issue among patients on maintenance hemodialysis (MHD), significantly impacting their quality of life and overall prognosis. While prior studies have reported variable prevalence rates globally, data specific to MHD patients in our regional tertiary care setting remain limited. This study addresses this gap byevaluating prevalence, severity, and associated factors of depression, thereby supporting evidence-based health strategies in this at-risk population. Methods: This cross-sectional study evaluated the prevalence and severity of depression in 74 patients undergoing MHD at a tertiary care center in North India. The Montgomery-Åsberg Depression Rating Scale (MADRS) was used to assess the symptoms of depression. Results: The overall prevalence of depression was 59.5%. Among the participants 33.8% had mild depression, 23.0% had moderate depression, and 2.7% had severe depression. Patients dialyzed via tunneled hemodialysis catheters exhibited significantly higher rates of depression compared to those with arteriovenous fistulas (p < 0.05). Patients with a transplant prospect had lower rates of depression compared to those without (p < 0.05). Conclusions: Depression is highly prevalent in patients on MHD. This study highlights the need for routine depression screening and appropriate management in this vulnerable population to improve their overall well-being and treatment outcomes.
Keywords: MHD; Depression; MADRS; AV fistula; Vascular access
Submitted: 11 July 2025; Accepted: 09 January 2026; Published: 20 June 2026
Authors for correspondence: Emails: jawadiqbal93@gmail.com
How to cite: Jawad Iqbal Rather, Amir Farooq, Muzamil Ahmad Wani, Nuha Saleem, Zeeza Hussain Shah, Muzafar Maqsood Wani, Imtiyaz Ahmad Wani, Imran Khan. Depression in prevalent maintenance hemodialysis patients. Journal of Renal and Hepatic Disorders. 2026; 10(1): 41-46. doi: 10.63268/jrenhp.v10i1.247.
DOI: 10.63268/jrenhp.v10i1.247
Copyright: The Author(s). Published by Troika Publisher. License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
Kidney diseases have a significant impact on global health. Chronic kidney disease (CKD) represents a significant and escalating global health challenge, with a worldwide prevalence estimated at 850 million individuals, corresponding to 14.2% of the global population [1]. The prevalence of CKD is projected to rise, driven by increasing rates of risk factors such as diabetes, hypertension, and obesity [2]. Major depressive disorder (MDD) is a prevalent mental health condition that affects over 332 million people worldwide. The lifetime prevalence of MDD is estimated at approximately 10.8%, and it contributes to an estimated 1 trillion USD in lost global productivity annually [3].
In patients receiving maintenance hemodialysis (MHD) for end-stage renal disease (ESRD), depression represents the most frequent psychiatric comorbidity, with an estimated prevalence ranging from 20% to 40%. Self- or clinician-administered questionnaires have been shown to detect depression more frequently than structured clinical interviews. A strong link between depression and increased mortality risk has been established among patients undergoing MHD [4]. Although affective and cognitive symptoms of depression may serve as more robust predictors of long-term mortality than somatic symptoms in MHD patients, depressive symptomatology independently contributes to dialysis nonadherence, increased healthcare resource utilization, and a reduced quality of life (QoL) [5].
Depression screening and management remain suboptimal within the dialysis population, despite its high prevalence and well-established impact on clinical outcomes [6]. Addressing this disparity is crucial for improving the overall well-being and survival outcomes of patients undergoing MHD.
The prevalence of depression and its associated factors may vary across the MHD population due to ethnic, socioeconomic, and clinical determinants. Evaluating these variables is essential to informing targeted interventions aimed at improving clinical outcomes and quality of life. Given the prevalence of depression remains largely uncharacterized in our specific MHD cohort, this study was conducted to assess the prevalence of depression in patients receiving MHD.
Materials and methods
This cross-sectional study was conducted between September 2024 and March 2025 at the Department of Nephrology, Sher-I-Kashmir Institute of Medical Sciences, Srinagar, India.
Patients aged ≥18 years who had been on maintenance hemodialysis for at least six months were included in the study. Patients with a pre-existing diagnosis of depression or any other psychiatric disorder, as well as those patients with hospitalization less than 2 months ago, were excluded.
A total of 74 patients were enrolled in the study. The sample size was determined using the formula for estimating a single population proportion: n = [Z2 × p(1 − p)]/d2, where Z = 1.96 (95% Confidence interval, CI), p = 0.5 (conservative estimate due to limited prior regional data), and d = 0.10, yielding an estimated sample size of approximately 96. The final sample size of 74, achieved through consecutive eligible enrollment over the study period, provided sufficient power for the primary prevalence endpoint (observed prevalence 59.5%).
A detailed history was taken, and a comprehensive general and systemic examination was performed. Patients were interviewed regarding various demographic related-factors, including rural versus urban dwelling, distance of hemodialysis center from the place of residence, number of medications per day, and whether accompanied by a caregiver to the hemodialysis center.
Assessment of the severity of depressive symptoms was performed using the Montgomery-Asberg Depression Rating Scale (MADRS), which is a 10-item rating scale where each item is scored from 0 to 6, resulting in a total score ranging from 0 to 60 [6]. The total MADRS score was obtained by summing the scores of all 10 items, with maximum possible score is 60. Higher scores indicate more severe depressive symptoms. Scors were interpreted as follows: 0 to 6—no depression, 7 to 19—mild depression, 20 to 34—moderate depression, 35 to 60—severe depression.
The primary aim of the study was to evaluate the prevalence and severity of depression in the study population.
Statistical methods
The data obtained was saved in Microsoft Excel 2024 (Microsoft, Redmond, WA, USA) and exported to the data editor of Statistical Package for Social Sciences (SPSS23, IBM, Armonk, NY, USA). Continuous variables were expressed as mean ± Standard deviation (SD), and categorical variables were expressed as frequencies and percentages. Data was presented in tabulated form. Fisher’s exact test was applied to compare categorical variables. A two-tailed p-value was used for calculating statistical significance, and p < 0.05 was considered statistically significant.
Results
A total of 74 patients were included in the study. The mean age of the patients was 52 (±14.2) years. Out of the 74 participants, 47 (63.5%) were males, and 27 (36.5%) were females. 40 (54.1%) patients belonged to the age group of 40–60 years. 66 (89.2%) had hypertension and 28 (37.8%) had a history of diabetes mellitus. The mean hemoglobin level was 7.9 (±1.3) g/dL. 52 (70.3%) patients were from a rural background. 56 (75.7%) patients had an arteriovenous fistula (AVF) as vascular access, while 18 (24.3%) had a tunneled hemodialysis catheter (HDC). The mean dialysis vintage was 20.8 (±15.0) months. The baseline parameters of the study population are presented in Table 1.
Table 1: Baseline characteristics of the study population.
| Parameter | Value | |
| Mean age (±SD) in years | 52 (±14.2) | |
| Gender, n (%) | ||
| Male | 47 (63.5%) | |
| Female | 27 (36.5%) | |
| Marital status, n (%) | Married | 58 (78.4%) |
| Comorbidities, n (%) | ||
| Hypertension | 66 (89.2%) | |
| Diabetes Mellitus | 28 (37.8%) | |
| Cardiovascular Disease | 7 (9.5%) | |
| Mean Hemoglobin g/dL (±SD) | 7.9 (±1.3) | |
| Residence, n (%) | ||
| Rural | 52 (70.3%) | |
| Urban | 22 (29.7%) | |
| Lifestyle factor n (%) | Active Smoker | 6 (8.1%) |
| Vascular access, n (%) | ||
| AVF | 56 (75.7%) | |
| Tunneled HDC (N (%)) | 18 (24.3%) | |
| Transplant Prospect (N (%)) | 15 (20.3%) | |
| Mean dialysis vintage (mon) (±SD) | 20.8 (±15.0) | |
| Mean distance of HD center from residence in kilometers (±SD) | 17.2 (±14.3) | |
| Accompanied by someone to Hemodialysis center (N (%)) | 72 (97.3%) | |
| Mean number of medications per day (±SD) | 7.7 (±2.3) | |
SD: standard deviation; AVF: arteriovenous fistula; HDC: hemodialysis catheter; HD: hemodialysis.
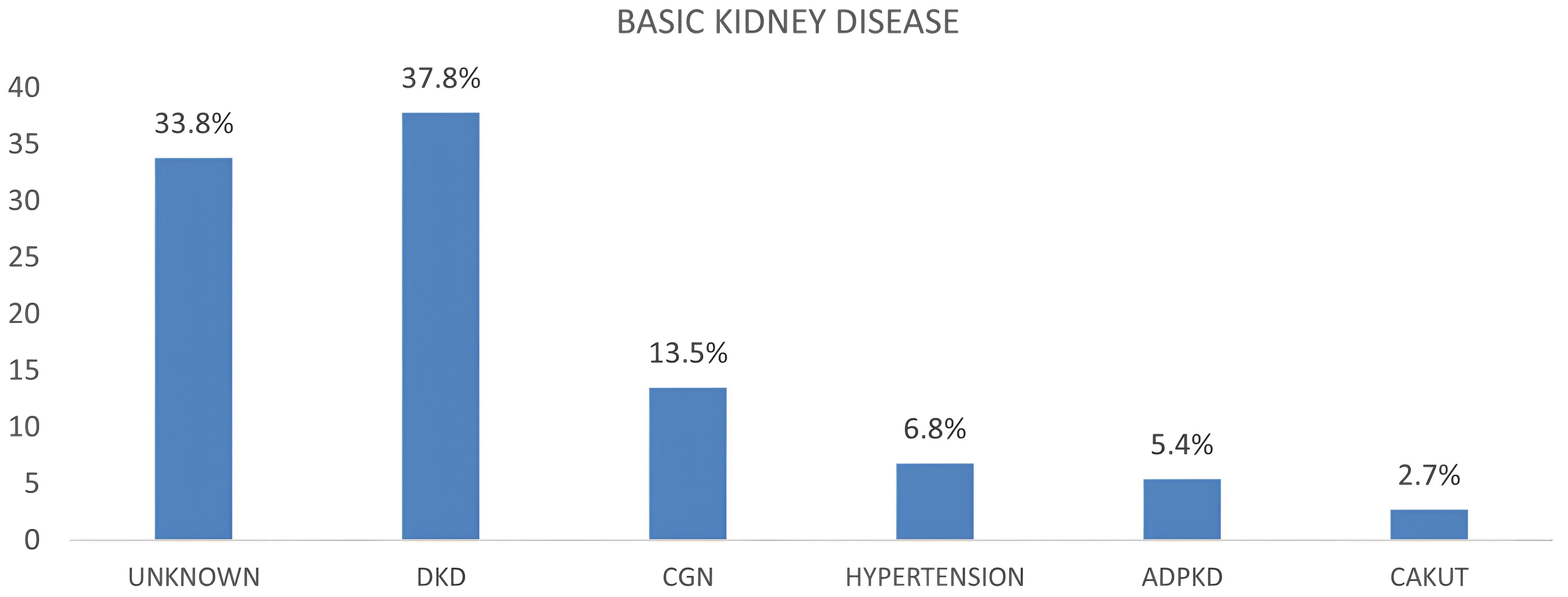
In terms of underlying kidney disease, 28 (37.8%) had diabetic kidney disease, followed by unknown etiology in 25 (33.8%), Fig. 1.
Figure 1 Etiology of kidney disease. DKD: diabetic kidney disease; CGN: chronic glomerulonephritis; ADPKD: adult dominant polycystic kidney disease; CAKUT: congenital abnormalities of the kidney and urinary tract.
Depression was identified in 44 (59.5%) patients based on MADRS score. Among these patients, 25 (33.8%) had mild depression, 17 (23.0%) had moderate depression, and 2 (2.7%) had severe depression, as shown in Table 2.
Table 2: Number of patients with and without depression (N = 74).
| Depression Severity | Frequency (n) | Percentage |
| No depression | 30 | 40.5 |
| Mild Depression | 25 | 33.8 |
| Moderate Depression | 17 | 23.0 |
| Severe Depression | 2 | 2.7 |
In subgroup analyses, age less than or more than 30 years of age was not associated with depression. Similarly, gender, marital status, urban vs. rural dwelling, or diabetes mellitus were not significantly associated with depression. Use of tunneled HDC was significantly associated with a higher rate of depression as compared with AVF as vascular access. On the other hand, patients who had a transplant prospect had lower rates of depression as compared to those without a transplant prospect, as shown in Table 3.
Table 3: Association of depression rates in various subgroups.
| Depression Present | No Depression | Fisher’s exact Test, p-Value | ||
| Age (yr) | ||||
| Age <30 | 4 | 4 | 0.707 | |
| Age ≥30 | 40 | 26 | ||
| Gender | ||||
| Male | 28 | 19 | >0.999 | |
| Female | 16 | 11 | ||
| Married | ||||
| Yes | 34 | 24 | >0.999 | |
| No | 10 | 6 | ||
| Dwelling | ||||
| Rural | 31 | 21 | >0.999 | |
| Urban | 13 | 9 | ||
| Diabetes Mellitus | ||||
| Yes | 19 | 9 | 0.331 | |
| No | 25 | 21 | ||
| Vascular access | ||||
| AVF | 27 | 29 | 0.001 | |
| Tunneled HDC | 17 | 1 | ||
| Transplant Prospect | ||||
| Yes | 5 | 10 | 0.037 | |
| No | 39 | 20 | ||
| Distance from home in Kilometers | ||||
| <20 | 23 | 10 | 0.153 | |
| ≥20 | 21 | 20 | ||
p-value of < 0.05 was taken as significant (Fisher’s Exact Test). AVF: arteriovenous fistula; HDC: hemodialysis catheter.
Discussion
Depression is one of the most common mental disorders in patients on MHD and is a frequently overlooked [7]. In the current study, 74 patients on MHD with a dialysis vintage of at least 6 months were evaluated for depression using the MADRS questionnaire.
The mean age of our study population was 52 (±14.2) years, which is consistent with other studies from India. Hockham et al. [8] conducted a multilevel analysis of the Nephroplus dialysis network across India and reported a median age of 53 years in the dialysis population. In our study, 47 (63.5%) participants were men, which aligns with other studies from India showing a gender disparity in access to hemodialysis [9, 10]. This contrast with studies from developed countries, where a higher percentage of women undergoing hemodialysis. In the Dialysis Outcomes and Practice Patterns Study (DOPPS), 41% of the study population were women [11]. The primary reason for this discrepancy may be explained by various sociocultural factors leading to decreased access to healthcare for women in India.
Twenty-eight patients (37.8%) of our study population had underlying diabetes mellitus, comparable to the study by Vijayan et al. [12], which included 897 hemodialysis patients, 335 (37.3%) had underlying diabetic kidney disease.
The mean hemoglobin concentration in our study was 7.9 (±1.3) g/dL. Modi et al. [13], reported that in the incident hemodialysis population, the mean hemoglobin concentration increased from 8.2 (±1.7) g/dL in 2002 to 9.1 (±1.7) g/dL in 2005. Since our study included a prevalent hemodialysis population with a minimum vintage of six months, these findings highlight the needs for better management of anemia. The mean dialysis vintage was 20.8 (±15) months.
Fifty-six patients (75.7%) had an AVF, which is comparable with other Indian studies Bansal D et al. [14] reported an AVF prevalence of 79% in the prevalent hemodialysis population. Fifty-two patients 52 (70.3%) were from a rural background. As per the Indian Chronic Kidney Disease (ICKD) study, two-thirds of the CKD patients in India reside in rural areas [15].
The mean distance of the hemodialysis center from the place of residence was 17.2 (±14.3) kilometers. In India, the distance is variable, ranging from >50 km in about 60% population [16] to around 5 km in other states [17].
The mean number of medications per day was 7.7 (±2.3). Julie et al. [18], in a study, including 176, 133 hemodialysis patients, reported a medication burden of 7.4 (±3.8) in 2013, which decreased to 6.8 (±3.6) in 2017. The appropriateness of medication prescription should be regularly assessed. This is necessary to prevent harm, futility, and unnecessary cost incursion due to inappropriate medication prescription.
The overall prevalence of depression in our study population, as measured by the MADRS questionnaire, was 59.5%. Reported prevalence of depression among patients on hemodialysis (HD) varies widely, ranging from 8% to 71% [19]. The varied prevalence of depression in this patient population may be attributed to differing patient demographics and different diagnostic criteria used for diagnosing depression. Using the MADRS scale in our study, 25 patients (33.8%) had mild depression, whereas 17 (23%) and 2 (2.7%) had moderate and severe depression, respectively.
The prevalence of depression was significantly higher in patients being dialyzed via tunneled HDC as compared with via AVF (p-value 0.001). Ahmet et al. [20], in their survey of 180 patients who were on hemodialysis, reported that the Beck Depression Inventory score of more than 14 (signifying the diagnosis of depression) was significantly higher in patients being dialyzed via tunneled cuffed HDC as compared to those being dialyzed via AVF. Patients who are being dialyzed via tunneled HDC have a lower quality of life, more frequent access dysfunction, increased need for vascular access interventions, and lower solute clearance than patients with a functional AVF. These factors may explain the increased prevalence of depression in patients on tunneled HDC [21].
Patients who were enrolled in the kidney transplant program had a significantly lower prevalence of depression compared with those who without a transplant prospect (p-value 0.03). Previous studies have reported that patients who have depressive symptoms have a lower chance of transplant listing [22].
Stratification as per age (less than or more than 30 years), gender, marital status, urban versus rural residence, diabetes status, or distance from home (more than or less than 20 kilometers) did not reveal a statistically significant difference in the prevalence of depression.
The pathophysiological mechanisms contributing to depression in patients on MHD are multifactorial. Biologically, progression of CKD is associated with accumulation of uremic toxins as well as inflammatory markers, such as interleukin-6 and tumor necrosis factor-alpha, which alter the neurotransmitter system and exert neurotoxic effects, contributing to depressive symptomatology. Additionally, dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis in ESRD leads to subclinical hypercortisolemia, further exacerbating mood disorders. Nutritional deficiencies, anemia, and altered body composition are frequently observed in MHD patients, may also contribute to depressive symptoms and reduced quality of life. Psychologically, the chronic stress of living with a life-altering condition, frequent dialysis sessions, physical limitations, and altered social roles contribute to emotional distress and depression [23].
This study highlights that depressive symptoms are highly prevalent in patients on MHD. These patients should be regularly screened for the symptoms of depression and actively managed. Depression in dialysis patients is associated with an increased risk of hospitalizations [24], withdrawal from dialysis [25], and all-cause mortality [4]. Hence, depression should be addressed in these patients to improve patient outcomes.
The limitations of our study include a small sample size, which may limit generalizability. Larger studies are needed from our patient population to confirm these findings. In addition, educational background and socioeconomic status were not assessed. Future studies should be done to assess the treatment outcome and efficacy of various therapies for depression in this patient population.
Conclusions
This study underscores the significant prevalence of depression among patients undergoing maintenance hemodialysis (MHD), with nearly 60% exhibiting depressive symptoms as measured by the MADRS questionnaire. Notably, the study identified a strong association between the use of tunneled hemodialysis catheters and higher rates of depression, as well as a protective effect linked to enrollment in kidney transplant programs. These findings highlight the critical need for routine depression screening and active management in MHD patients, given the known negative impacts of depression on hospitalization rates, dialysis withdrawal, and overall mortality. Although the study is limited by its small sample size and the lack of assessment of socioeconomic factors, necessitate further investigation through larger, more comprehensive studies, it provides valuable insight into the mental health challenges faced by this vulnerable population. Future research should evaluate the effectiveness of various therapeutic interventions for depression in MHD patients, with the ultimate goal of improving patient outcomes and quality of life.
Availability of data and materials
The data is available and can be assessed on a reasonable request.
Author contributions
JIR—designed the concept, collected data, and wrote the manuscript. AF and MAW—helped in data collection and analysis. NS and ZHS—helped in data collection. MMW, IAW and IK—critically reviewed the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
This study was approved by the institutional ethics committee SKIMS. The protocol number is 123/2024. Written informed consent was taken from the study participants.
Acknowledgment
We acknowledge the contribution of patients, residents, and the dialysis staff who made this study possible.
Funding
This research received no external funding.
Conflict of interest
The authors declare no conflict of interest.
REFERENCES
1. GBD 2023 Chronic Kidney Disease Collaborators. Global, regional, and national burden of chronic kidney disease in adults, 1990–2023, and its attributable risk factors: a systematic analysis for the Global Burden of Disease Study 2023. The Lancet. 2025; 406: 2461–2482.
2. Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney International Supplements. 2022; 12: 7–11.
3. Rong J, Wang X, Cheng P, Li D, Zhao D. Global, regional and national burden of depressive disorders and attributable risk factors, from 1990 to 2021: results from the 2021 Global Burden of Disease study. British Journal of Psychiatry. 2025; 227: 688–697.
4. Zhao J, Wu M, Zhang L, Han X, Wu J, Wang C. Higher levels of depression are associated with increased all-cause mortality in individuals with chronic kidney disease: a prospective study based on the NHANES database. Journal of Affective Disorders. 2025; 390: 119785.
5. Wicke FS, Ernst M, Otten D, Werner A, Dreier M, Brähler E, et al. The association of depression and all-cause mortality: explanatory factors and the influence of gender. Journal of Affective Disorders. 2022; 303: 315–322.
6. Fischer MJ, Streja E, Hsiung JT, Crowley ST, Kovesdy CP, Kalantar-Zadeh K, et al. Depression screening and clinical outcomes among adults initiating maintenance hemodialysis. Clinical Kidney Journal. 2021; 14: 2548–2555.
7. Kubanek A, Renke M, Godlewska BR, Paul P, Przybylak M, Kowalska AS, et al. Screening for depression in chronic haemodialysis patients as a part of care in dialysis setting: a cross-sectional study. Frontiers in Psychiatry. 2024; 15: 1410252.
8. Hockham C, Ghosh A, Agarwal A, Shah K, Woodward M, Jha V. Centre-level variation in the survival of patients receiving haemodialysis in India: findings from a nationwide private haemodialysis network. The Lancet Regional Health—Southeast Asia. 2024; 23: 100383.
9. Mharapara P, Ahmed SB, Olson J, Schick-Makaroff K. Sex and gender characteristics of adults on hemodialysis experiencing depression and depressive symptoms: a scoping review. Canadian Journal of Kidney Health and Disease. 2025; 12: 20543581251378018.
10. Shaikh M, Woodward M, John O, Bassi A, Jan S, Sahay M, et al. Utilization, costs, and outcomes for patients receiving publicly funded hemodialysis in India. Kidney International. 2018; 94: 440–445.
11. Hecking M, Bieber BA, Ethier J, Kautzky-Willer A, Sunder-Plassmann G, Säemann MD, et al. Sex-specific differences in hemodialysis prevalence and practices and the male-to-female mortality rate: the Dialysis Outcomes and Practice Patterns Study (DOPPS). PLOS Medicine. 2014; 11: e1001750.
12. Vijayan M, Radhakrishnan S, Abraham G, Mathew M, Sampathkumar K, Mancha NP. Diabetic kidney disease patients on hemodialysis: a retrospective survival analysis across different socioeconomic groups. Clinical Kidney Journal. 2016; 9: 833–838.
13. Modi GK, Jha V. The incidence of end-stage renal disease in India: a population-based study. Kidney International. 2006; 70: 2131–2133.
14. Bansal D, Kher V, Gupta KL, Banerjee D, Jha V. Haemodialysis vascular access: current practices amongst Indian nephrologists. The Journal of Vascular Access. 2018; 19: 172–176.
15. Kumar V, Yadav AK, Sethi J, Ghosh A, Sahay M, Prasad N, et al. The Indian Chronic Kidney Disease (ICKD) study: baseline characteristics. Clinical Kidney Journal. 2021; 15: 60–69.
16. Dare AJ, Fu SH, Patra J, Rodriguez PS, Thakur JS, Jha P; Million Death Study Collaborators. Renal failure deaths and their risk factors in India 2001-13: nationally representative estimates from the Million Death Study. The Lancet Global Health. 2017; 5: e89–e95.
17. Sahay M, Ismal K, Vali PS. Hemodialysis at doorstep—“Hub-and-Spoke” model of dialysis in a developing country. Saudi Journal of Kidney Diseases and Transplantation. 2020; 31: 840–849.
18. Paik JM, Zhuo M, York C, Tsacogianis T, Kim SC, Desai RJ. Medication burden and prescribing patterns in patients on hemodialysis in the USA, 2013–2017. American Journal of Nephrology. 2021; 52: 919–928.
19. Chilcot J, Wellsted D, Da Silva-Gane M, Farrington K. Depression on dialysis. Nephron Clinical Practice. 2008; 108: c256–c264.
20. Çora AR, Çelik E. Association between vascular access type and depression in hemodialysis patients. Hemodialysis International. 2023; 27: 296–300.
21. Keser BN, Kirman UN, Kocaaslan C, Aydin E. The association between vascular access type and depressive symptoms in geriatric hemodialysis population. Vascular. 2020; 28: 390–395.
22. Chen X, Chu NM, Basyal PS, Vihokrut W, Crews D, Brennan DC, et al. Depressive symptoms at kidney transplant evaluation and access to the kidney transplant waitlist. Kidney International Reports. 2022; 7: 1306–1317.
23. Yuan C, Chang F, Zhai H, Du J, Lu D, Ma H, et al. Integrative approaches to depression in end-stage renal disease: insights into mechanisms, impacts, and pharmacological strategies. Frontiers in Pharmacology. 2025; 16: 1559038.
24. Hedayati SS, Grambow SC, Szczech LA, Stechuchak KM, Allen AS, Bosworth HB. Physician-diagnosed depression as a correlate of hospitalizations in patients receiving long-term hemodialysis. American Journal of Kidney Diseases. 2005; 46: 642–649.
25. Lopes AA, Albert JM, Young EW, Satayathum S, Pisoni RL, Andreucci VE, et al. Screening for depression in hemodialysis patients: associations with diagnosis, treatment, and outcomes in the DOPPS. Kidney International. 2004; 66: 2047–2053.