
Download
Review
The oncogenic implications of metabolic dysfunction-associated steatotic liver disease
Aditya Kamboj1, Amit Kumar Singh1,*
1Department of Medical Lab Technology, UIAHS, Chandigarh University, 140301 Mohali, India
Abstract
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly termed non-alcoholic fatty liver disease (NAFLD), is receiving growing attention as a major public health issue globally, primarily because of its association with the development of hepatocellular carcinoma (HCC). MASLD is predominantly caused by obesity, type 2 diabetes mellitus, and lack of exercise, and has a broad clinical spectrum ranging from benign hepatic steatosis to non-alcoholic steatohepatitis (NASH), fibrosis, cirrhosis, and ultimately HCC. The pertinent problem is that HCC due to MASLD typically develops in patients without cirrhosis, making diagnosis and follow-up exceedingly challenging. MASLD is described as a multi-faceted condition involving insulin resistance, lipid deposition, oxidative stress, and chronic inflammation. Recent molecular studies related to lipid metabolism, mitochondrial dysfunction, and oncogenic pathways have identified candidate molecules, including microRNA-33 (miR-33), and Interferon Gamma Inducible Protein 16 (IFI16) variants. Emerging non-invasive diagnostic technologies, including liquid biopsies, next-generation sequencing (NGS), and machine learning-based models, are becoming important for early detection and individualized risk assessment. Currently, therapeutic interventions target oxidative stress, inflammatory responses, fibrosis, and lipid dysregulation. Some of the potentially useful interventions include bioactive flavonoids, repurposed medications (metformin and statins), and a novel nanotechnology-based drug delivery system that could slow disease progression and reduce cancer risk. Treating MASLD while addressing the risk of malignancy will require a precision medicine approach with a focus on lifestyle intervention, directed pharmacotherapy, and advanced diagnostic approaches implemented in a multidisciplinary fashion.
Keywords: Non-alcoholic fatty liver disease (NAFLD); Non-alcoholic steatohepatitis (NASH); Metabolic dysfunction-associated steatotic liver disease (MASLD); Metabolic dysfunction-associated steatohepatitis (MASH); Hepatocellular carcinoma (HCC)
Submitted: 09 October 2025; Accepted: 24 December 2025; Published: 20 June 2026
Authors for correspondence: Emails: amit.e15899@cumail.in
How to cite: Aditya Kamboj, Amit Kumar Singh. The oncogenic implications of metabolic dysfunction-associated steatotic liver disease. Journal of Renal and Hepatic Disorders. 2026; 10(1): 14-23. doi: 10.63268/jrenhp.v10i1.252.
DOI: 10.63268/jrenhp.v10i1.252
Copyright: The Author(s). Published by Troika Publisher. License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
Metabolic dysfunction-associated fatty liver disease (MAFLD), earlier known as non-alcoholic fatty liver disease (NAFLD), is now a critical global health concern because of its robust association with cancer etiology. Increasing evidence has placed the spotlight on MASLD as a primary causative factor not only for liver cancer but also for extrahepatic cancers. Most importantly, it has been strongly established as a leading risk factor for hepatocellular carcinoma (HCC), the increasing prevalence of which is closely associated with the global increase in metabolic disorders [1]. Its prevalent nature is owed mainly to increasingly sedentary lifestyles, low levels of physical activity, and the chronic intake of high-calorie diets that tend to exceed the body’s energy requirements, especially when linked with poor dietary quality and food imbalance [2]. The defining feature of this condition is the accumulation of fat in the liver in the absence of other contributing factors, such as significant alcohol consumption. Obesity, type 2 diabetes mellitus, and metabolic syndrome have consistently been identified as its primary risk factors [3]. The global surge in obesity and type 2 diabetes has paralleled a sharp rise in the prevalence of MASLD. Recent data indicate that approximately 38% of the adult population is affected, while rates among children and adolescents range between 7% and 14%. Projections suggest that by 2040, nearly 55% of the world’s population could be living with MASLD. Although not every individual with the condition will progress to advanced liver disease, MASLD has nonetheless emerged as the leading indication for liver transplantation in the United States, particularly among women and those diagnosed with hepatocellular carcinoma (HCC) [4]. Although the genetic determinants of hepatic fat accumulation, such as allelic variants of lipid metabolism genes, may also play a role, these are less common and more frequent risk factors such as obesity and components of metabolic syndrome are more frequent. The prevalence of nonalcoholic fatty liver disease (NAFLD) without obesity widely ranges, suggesting that exogenous factors (such as high cholesterol, consumption of sugars such as fructose) and genetic risk factors both contribute to the development of NAFLD, but the latter is not a primary cause [5]. Histologically, NAFLD may be classified into two primary groups: nonalcoholic steatohepatitis (NASH) and nonalcoholic fatty liver (NAFL). Lack of hepatic damage, notably ballooning degeneration in hepatocytes, and the buildup of fat in the liver are characteristics of NAFL. NASH, on the other hand, is characterized by hepatic steatosis, inflammation, and visible hepatocyte damage, including ballooning and may occur with or without fibrosis [6].
Even though there is increasing evidence of the association between MAFLD and both hepatic and extrahepatic cancers, several important questions remain unanswered. The majority of the literature remains highly concentrated on HCC, and the potential mechanisms linking MAFLD to cancers beyond the liver are not yet fully understood. It is also challenging to determine causal relationships and patterns of cumulative risk progression, especially in diverse global populations, because large-scale longitudinal studies are seldom available [7]. Unresolved questions include the extend to which disease severity, particularly fibrosis stage, directly impacts cancer incidence, whether MAFLD is an independent driver of carcinogenesis or merely a reflection of underlying metabolic dysfunction, and whether early targeted interventions could potentially significantly reduce future cancer risk in this patient population [8]. The role of MAFLD in clinical response to cancer therapy, and treatment efficacy and outcomes, remain poorly defined, and further mechanistic and clinical research is needed to understand its role [9]. Thus, this review provides a comprehensive summary of the literature on MAFLD and liver-related or extra-hepatic cancers with primary focus on recent knowledge gaps between MAFLD and cancer development, identifies major scientific hurdles as well as clinical needs based on current understanding, and proposes future research directions ranging from molecular mechanisms to advanced risk-stratification models and population-specific longitudinal studies, aimed to developing effective cancer prevention strategies secondary to MAFLD.
Metabolically driven steatotic liver disorder
Perspective and terminology
Fatty liver associated with is well known to cause liver damage and, in more extreme cases, to progress to cirrhosis. NASH was first identified as an independent liver-damaging condition in the 1980’s, and was subsequently named by researchers [10]. The term NAFLD covers a spectrum of chronic liver diseases, ranging from simple hepatic steatosis (NAFL) to non-alcoholic steatohepatitis (NASH), which involves inflammatory and injurious changes of the liver, with or without fibrosis [11]. This condition was reclassified as MAFLD in 2020 after decades of research on MAFLD and its mechanisms underwent thorough investigation, showing evidence that implicates MAFLD in affecting systems outside of the liver. MAFLD is diagnosed when there is evidence for excess liver fat (which can be quantified via biopsy, imaging, or biomarker) in conjunction with at least one of the following overweight or obesity, type 2 diabetes mellitus, or displaying symptoms of metabolic dysfunction [2]. With the change in naming conventions, MASLD is now a diagnosis based on inclusion and not necessarily exclusion of other causes. In 2023, the terminology was revised again to MASLD, which represents the disease with its connection to cardiometabolic disorders and shared underlying biological mechanisms [12].
Etiopathogenesis
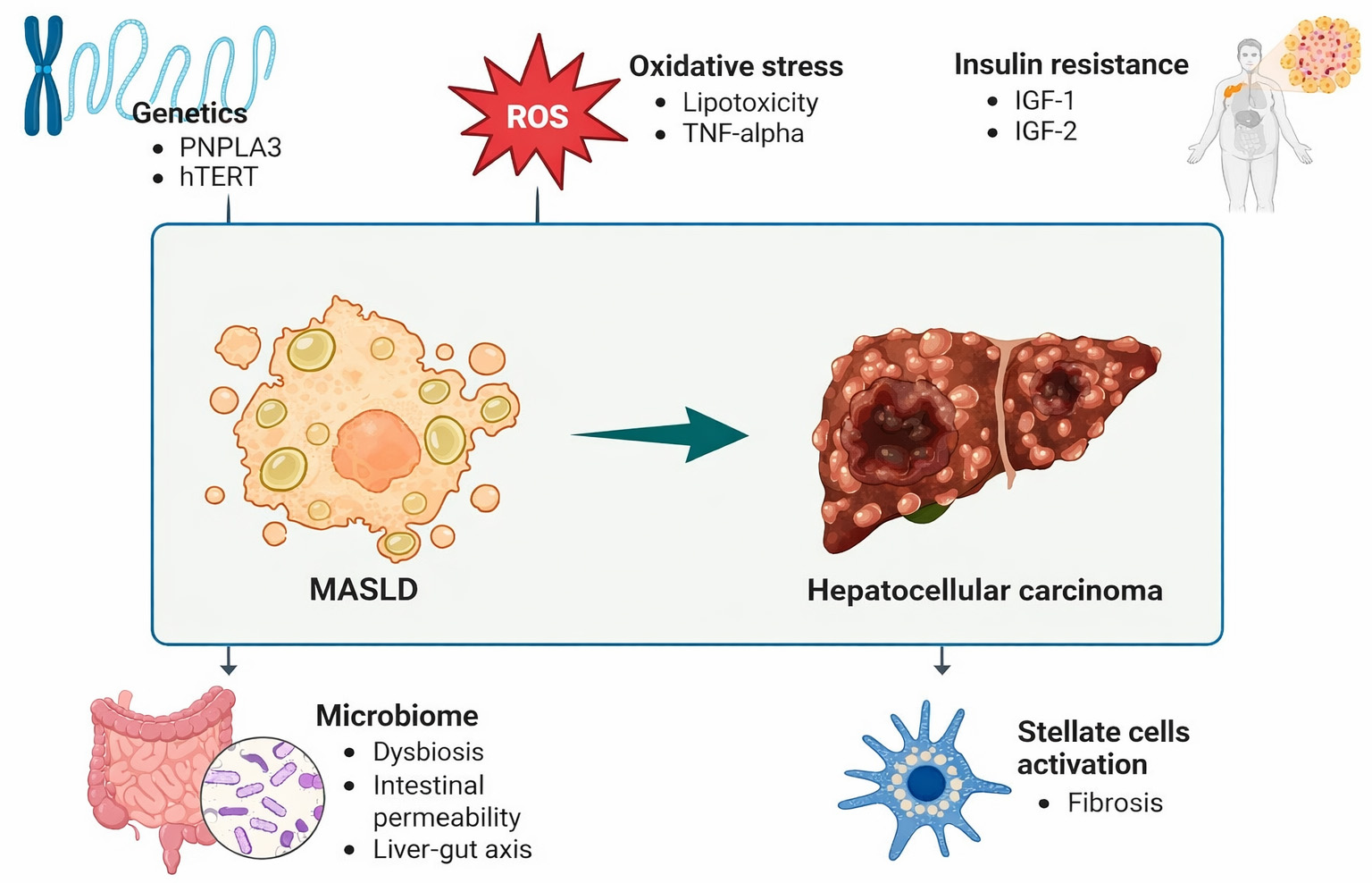
It is important to fully understand the epidemiology of MASLD, as its increasing global prevalence and significant metabolic associations have made it one of the most common causes of chronic liver disease worldwide [13]. Studies have repeatedly found a clear link between metabolic syndrome and MASLD. However, the causes and how the disease develops in MASLD are not well understood. The “two-hit” hypothesis (first proposed in NAFLD) states that the first hit (mostly hepatic steatosis due to insulin resistance and other contributing factors) sensitizes the liver, while a second hit (including oxidative stress, inflammatory cytokines, mitochondrial dysfunction) leads to inflammation, cell death, and fibrosis [14]. In contrast, the “multiple-hit” (or multi-hit) hypothesis argues that this model is too simplistic. Rather than just two sequential hits, many insults act in parallel on a liver that is genetically predisposed to injury, such as insulin resistance, adipokines that act from adipose tissue, gut microbiota, dietary/nutritional factors, genetic and epigenetic predispositions, endoplasmic reticulum (ER) stress, lipotoxicity [15]. The “multiple hits” model suggests that MASLD develops in people who have a genetic tendency to develop it and are also exposed to several environmental factors, such as lifestyle behaviors, dietary patterns, and the bacteria in their gut (Fig. 1, Ref. [16]). Importantly, hypotheses apply to mechanisms that involve carbohydrate and fat metabolism, and insulin resistance, such as the increased production of fat in the liver (de novo lipogenesis), reduced regulation of the breakdown of fat in adipose tissue (e.g., increased fatty acid release and reduced breakdown of fatty acids), all of which contribute to lipotoxicity [17].
Figure 1 Schematic representation of the pathways progression of MASLD to hepatocellular carcinoma, involving genetic susceptibility, oxidative stress, insulin resistance, gut microbiome disturbances, and activation of stellate cells leading to fibrosis [16]. https://www.mdpi.com/2077-0383/13/16/4657. PNPLA3: Patatin-like phospholipase domain-containing protein 3; hTERT: telomerase reverse transcriptase (in human); MASLD: Metabolic dysfunction-associated steatotic liver disease; TNF: Tumor necrosis factor; IGF: insulin-like growth factors.
Pathophysiology of MASLD-HCC
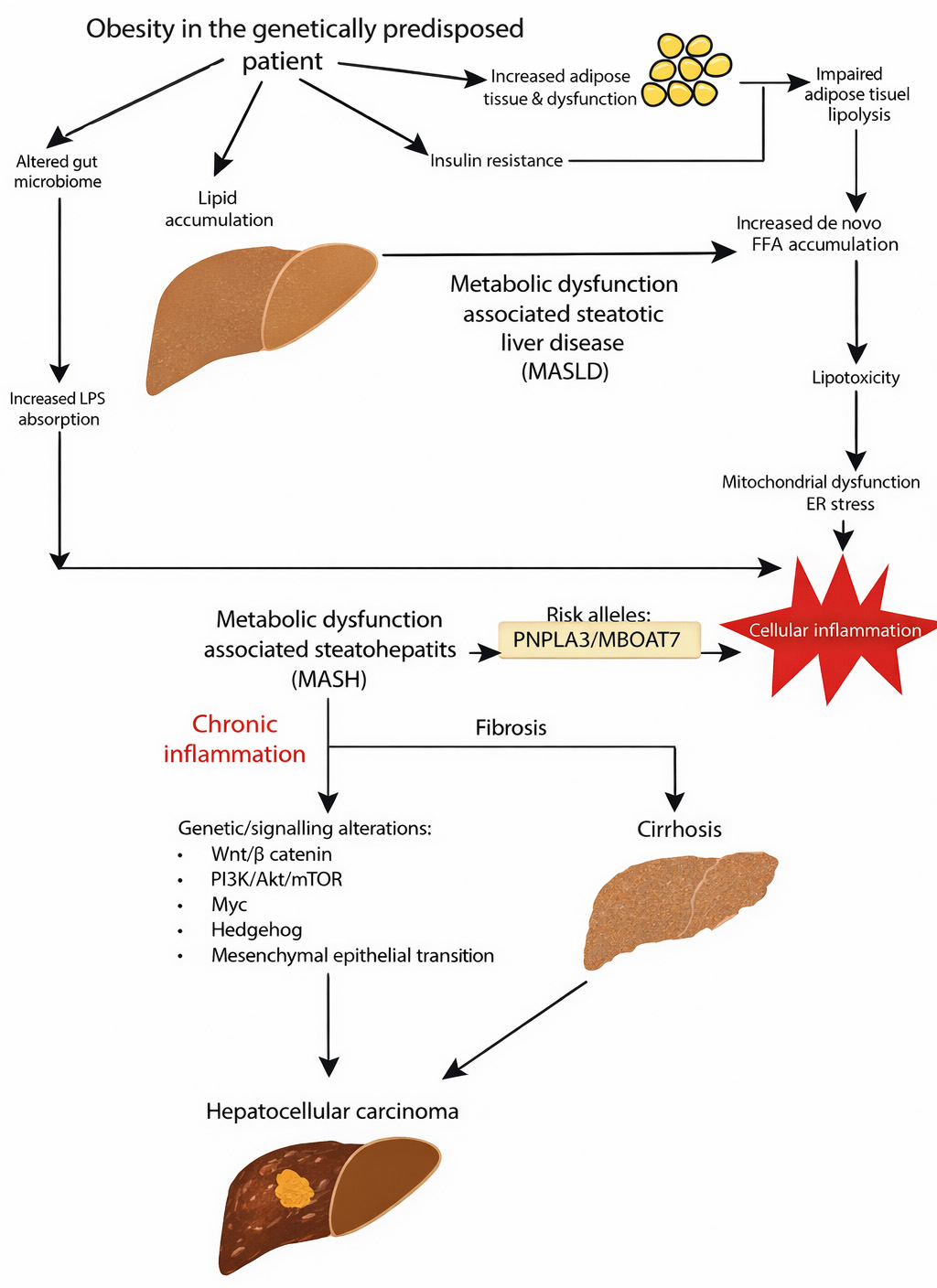
The pathogenesis of MASLD is intricate and multifaceted, encompassing fibrogenesis, lipotoxicity, and inflammatory pathways. Following food intake, elevated blood glucose levels stimulate pancreatic insulin secretion; this is an important phase of operation. Then, insulin travels via the portal vein to the liver, where it directs metabolic pathways such as increasing de novo lipogenesis, which converts acetyl-coenzyme A (CoA) into fatty acids, and stimulates glycogenesis, storing excess glucose as glycogen. Activated by insulin, several intracellular signaling pathways mediate these anabolic actions. By managing oxidative metabolism, adenosine triphosphate (ATP) synthesis, and reactive oxygen species production, mitochondria play a crucial part in metabolic regulation. Increased hepatic lipogenesis, decreased insulin signaling in adipose tissue, and increased free fatty acid levels are all consequences of dysregulated anabolic signaling in the setting of hepatic insulin resistance. The development of MASLD is primarily dependent on the accumulation of fatty acids in the liver, which is largely caused by increased lipogenesis triggered by specific transcription factors. Fatty acid β-oxidation, which occurs in the mitochondria of the liver, transforms fatty acids into triglycerides, which are then encapsulated in very-low-density lipoproteins (VLDL) and secreted into the bloodstream. Hepatic steatosis results from triglycerides building up as lipid droplets inside hepatocytes when the capacity for either lipid export or oxidation is surpassed [18]. The development of HCC in MASLD is complicated. Fig. 2 (Ref. [19]) illustrates possible pathways. In liver cells, the accumulation of fat with an underlying lipotoxicity produces a persistent state of inflammation that, over time, leads to fibrosis [19].
Figure 2 Pathogenic mechanisms linking obesity, genetics, insulin resistance, and inflammation to Metabolic dysfunction-associated steatotic liver disease (MASLD) progression, fibrosis, cirrhosis, and hepatocellular carcinoma [19]. https://www.mdpi.com/2072-6694/16/2/259. LPS: Lipopolysaccharides; FFAs: Free fatty acids; PNPLA3: Patatin-like phospholipase domain-containing protein 3; MBOAT7: membrane-bound O-acyltransferase domain-containing 7; Myc: myelocytoma; Wnt: Wingless/Integrated; PI3K: Phosphoinositide 3-Kinase; Akt: Protein Kinase B; mTOR: mechanistic Target of Rapamycin; ER: Endoplasmic reticulum.
MASLD as a spectrum: from steatosis to NASH and fibrosis
Lipid accumulation within hepatocytes characterize both disorders, however, their histological features, propensity for disease development, and clinical prognosis differ significantly. When fat is present in over 5% of hepatocytes without significant inflammation or hepatocellular damage, NAFL is recognized. It has always been thought to be a non-progressive, mostly benign illness. Emerging data, however, casts doubt on this presumption, suggesting that this oversimplified viewpoint could ignore the danger in some subgroups. Particularly in the presence of metabolic comorbidities such as obesity and type 2 diabetes mellitus, between 25–30% of individuals with NAFL may progress to fibrosis and a subgroup to NASH. However, in addition to steatosis, NASH is typified by lobular inflammation and hepatocyte damage, including ballooning degeneration. This kind of illness has a much higher chance of developing cirrhosis, severe fibrosis, and HCC. It has been determined that the degree of fibrosis is the most accurate indicator of liver-related morbidity and overall mortality among several histological characteristics. Since a liver biopsy is now required for a definite diagnosis, distinguishing between NAFL and NASH is still clinically difficult. Disease monitoring and risk assessment are made more difficult by the fact that non-invasive diagnostic techniques still lack the sensitivity and specificity to reliably differentiate between the two. Advancing research identifies the wider systemic effect of NAFLD, which indicates that even individuals with uncomplicated steatosis are susceptible to drug-induced liver damage, alcoholic liver injury, and cardiovascular disturbances likely due to underlying hepatocellular dysfunction [20].
Epidemiological link between MASLD and cancer
MASLD has been the fastest-increasing cause of HCC globally. A Swedish population-based study is presented as recent evidence that MASLD has surpassed conventional causes of hepatitis C virus (HCV) infection as the leading cause of HCC in Sweden. Between 2012 and 2018, the incidence of MASLD-related HCC increased markedly, rising by 50% from 1.0 to 1.5 cases per 100,000 person-years. By 2017, MASLD accounted for 22% of all diagnosed cases of HCC in Sweden, overtaking HCV as the most common underlying cause. The declining prevalence of viral hepatitis due to successful antiviral therapy and the rising global prevalence of obesity, type 2 diabetes, and metabolic syndrome are two of the large burden diseases with a high risk of MASLD, and are only two illustrations of the broader shifts in disease epidemiology underlined by this trend. The study found that 39% of MASLD related HCC did not have cirrhosis, which is particularly clinically relevant. The exclusion of non-cirrhotic people from existing monitoring techniques usually results in delayed diagnosis, a higher tumor burden, and limited access to curative treatment choices, which makes this study noteworthy. Although early-stage detection rates (Barcelona Clinic Liver Cancer (BCLC) stage 0–A) were similar, individuals with MASLD-HCC were often older (median age of 75), had bigger tumors, and had a greater risk of extrahepatic metastases than patients with HCC from other sources. Relative to their non-MASLD counterparts, a lower percentage of MASLD-HCC patients received curative therapy; however, after controlling for confounding factors, adjusted multivariable analysis showed no statistically significant differences in outcomes. The need to develop more comprehensive monitoring systems and improve HCC risk classification is highlighted by these findings, especially for MASLD, those who have no evidence of cirrhosis but are nonetheless at high risk for liver cancer [21].
Molecular and genetic mechanisms linking MASLD to cancer
The research, “miR-33 deletion in hepatocytes attenuates MASLD-MASH-HCC progression”, examines the molecular and genetic pathways responsible for the progression of hepatocellular carcinoma (HCC) from MASLD. This study examines the role of microRNA-33 (miR-33) because it has been identified as a key regulator of liver disease development from metabolism. Hepatocellular carcinoma (HCC) and liver fibrosis are serious outcomes of the most common liver disease, known as MASLD. Researchers reported that miR-33 levels were demonstrably elevated in the livers of MASLD patients and in animals used in experiments. The authors made a miR-33 knockout mouse model in hepatocytes available for a deeper understanding as well. The miR-33 knockout mice exhibited some significant metabolic disruptions, such as inhibiting liver fat condensation, promoting reduced inflammation, and limiting fibrotic developments. The cellular consequences of the knockdown of miR-33 included inhibition of lipogenesis, stimulation of mitochondrial biogenesis, and stimulation of fatty acid oxidation. It also upregulated genes involved in cholesterol regulation and antioxidant defense, and downregulated pathways of liver damage and injury. It is interesting to note that deletion of miR-33 downregulates the yes-associated protein/transcriptional co-activator with PDZ-binding motif (YAP/TAZ) signaling pathway, which is a major driver of liver cancer development. Long-term experiments demonstrated a significant reduction in liver tumors in miR-33-deficient mice, in addition to inhibition of tumor growth and cell proliferation. Overall, miR-33 is a molecular link between metabolic liver disease and cancer and represents a potential therapeutic target for preventing MASLD-associated HCC [22]. The majority of existing data on miR-33 in NAFLD comes from preclinical models. For example, in fructose-fed mice, hepatic miR-33 is altered, and functional studies are performed using in vitro [23].
Diagnostic and biomarker strategies
Through an integrated analysis of RNA sequencing states and whole-exome sequencing of liver tissues from patients with MASLD, three distinct transcriptomic subtypes (G1–G3) have been identified, which reflect differences in the stage of disease progression. The IFI16 gene variant (rs6940, A>T, portending a missense mutation T779S), represents an important factor associated with worsening disease severity. This variant enhances inflammatory responses through DNA-sensing, specially via the interferon gamma inducible protein 16 IFI16-PYCARD (adaptor protein that is composed of two protein-protein interaction domains: a N-terminal PYRIN-PAAD-DAPIN domain (PYD) and a C-terminal caspase-recruitment domain (CARD))-protease enzyme Caspase-1 (CASP1) signaling pathway, which can act as a biomarker of disease progression for MASLD [24]. In relation to IFI16, the data is more in the early stages. A very recent integrative genomic/transcriptomic study in MASLD liver tissue reported that genetic variants for IFI16 (rs6940) had associations with disease progression, and that in vitro binding assessments indicated the variant had stronger dsDNA binding and increased inflammatory signaling through the IFI16-PYCARD-caspase-1 pathway [24]. Next-generation sequencing (NGS) and artificial intelligence (AI) advancements are revolutionizing the diagnosis and management of HCC. Alpha-fetoprotein (AFP) testing and ultrasound imaging are traditional methods that have been undervalued, as they are not sensitive, particularly at the earlier stages of disease detectable by the testing modalities. NGS allows for the capacity of identifying a genetic mutation in somatic blood or tissue to allow early diagnosis. In particular, non-invasive liquid biopsies (specifically those making the distinction between circulating tumor DNA and cfDNA) are being increasingly recognized for their reliable potential for the early, accurate diagnosis as technologists increasingly trust the sufficiency of the data. Commercially available platforms such as Foundation One Liquid CDx and Guardant360 CDx, now provide timely, safe, and more precise alphanumeric characterization results. In addition to diagnosis, NGS also identifies molecular biomarkers, which are crucial for personalized treatment. NGS makes it possible to identify resistance-associated mutations in viral hepatitis, such as Hepatitis B Virus (HBV) and HCV (e.g., G1896A in HBV; (Nonstructural protein 5A) NS5A and NS5B mutations in HCV), which helps choose antiviral treatments that work.
Furthermore, changes in Tumor Protein p53 (TP53), Telomerase Reverse Transcriptase (TERT), and Catenin Beta 1 (CTNNB1) are examples of recurrent somatic mutations in HCC that have therapeutic and prognostic consequences. For example, CTNNB1 mutations may indicate resistance to immunotherapy, especially immune checkpoint drugs, but TP53 mutations are frequently linked to poor clinical outcomes. Through the analysis of intricate genomic datasets, AI greatly enhances the usefulness of NGS by identifying molecular patterns and mutations that are clinically significant. Invasive treatments are frequently avoided because of AI-based diagnostic algorithms that improve early detection and make accurate variant calling possible. The integration of NGS with AI thus supports a precision oncology framework, allowing for more tailored treatment plans and better patient outcomes [25].
Prognostic modeling for MASLD-related HCC
Several recent investigations have aimed to delineate the differences between patients with and without cirrhosis regarding the incidence and clinical outcomes of HCC developing in association with MASLD. Nearly 35% of cases of HCC associated with MASLD develop in non-cirrhotic livers, according to data from a multicenter registry. The non-cirrhotic MASLD-related HCC patients tend to have larger tumor sizes (as well as more advanced stages of disease) and were often older at diagnosis compared to cirrhotic patients, but also had better liver function, with the consideration that they may receive more aggressive and potentially curative therapies. Since HCC typically presents incidentally in non-cirrhotic patients, they are not routinely surveilled, and as such, their diagnosis is generally at a later stage of disease than their cirrhotic counterparts. As a result of their higher hepatic functional reserve, non-cirrhotic MASLD patients can achieve survival outcomes similar to patients with cirrhosis, even if they tend to have a greater burden of tumor [23, 24]. In addition, research shows that while the overall incidence of HCC in MASLD patients without cirrhosis is low (<1.5 cases per 1000 patient years), it is still clinically relevant, given how common MASLD is worldwide [23]. Although the primary aim of present screening initiatives is aimed at cirrhotic patients, this distinction has significant consequences for surveillance approaches. Robust predictive models and extensive cost-benefit analyses are needed to adequately incorporate non-cirrhotic MASLD [25]. Table 1 (Ref. [21, 26, 27, 28, 29]) summarizes key studies detailing the study type, country, duration, and major findings, providing an evidence-based overview of the oncogenic risk associated with MASLD.
Table 1: Overview of key studies examining MASLD associated cancer risk.
| S/N | Methodology/study design/case details | Country | Duration/follow-up | Major findings & notes | References |
| 1 | Narrative + systematic synthesis of human studies on HCC arising in MASLD; analyzed epidemiology, surveillance issues, and non-cirrhotic HCC cases | USA/international literature | NA (review) | MASLD is an increasingly common cause of HCC; up to ~30% of MASLD-related HCC occurs in non-cirrhotic livers, with implications for surveillance strategies. | [26] |
| 2 | Prospective cohort analysis using UK Biobank baseline data; SLD subtyping into MASLD, MetALD, and other categories; multivariable Cox models for 24 site-specific cancers | United Kingdom | 283,238 participants; median follow-up reported in cohort (see paper) | MASLD was the most prevalent SLD and associated with increased risk of overall cancer, digestive system cancers (except gastric), breast cancer, renal and endometrial cancers and Hodgkin lymphoma; estimated PAR% higher for MASLD for many cancers. | [27] |
| 3 | Large population cohort using national health records; fatty-liver indices to classify SLD subtypes; Fine–Gray subdistribution hazards for cancer risk across millions of person-years | South Korea | Very large sample; multi-year follow-up (tens of millions of person-years) | MASLD, MetALD and other SLDs linked to higher liver and GI cancer risk; MetALD showed particularly high risk; MASLD linked to modest increases in some extrahepatic cancers. | [26] |
| 4 | Nationwide registry analysis of HCC etiology trends; categorized HCC cases by underlying cause (MASLD, viruses, alcohol) | Sweden | National registry years (longitudinal) | MASLD became the most common cause of HCC in Sweden over the study period—demonstrating a epidemiological shift from viral to metabolic drivers. | [21] |
| 5 | Meta-analysis pooling longitudinal cohorts comparing NAFLD vs. non-NAFLD for HCC incidence and mortality; subgroup analyses by fibrosis/NASH | Multi-country (studies pooled internationally) | Varied follow-up across included cohorts | NAFLD (and especially NASH with fibrosis) was associated with increased HCC incidence and liver-cancer mortality—supporting fibrosis stage as a key predictor. | [28] |
| 6 | Longitudinal cohort assessing dynamic changes in MASLD/steatosis status and subsequent HCC risk; adjusted for metabolic factors and medications | Multi-cohort/pooled data | Several years per subject (cohort dependent) | Changes in MASLD status over time predicted differential HCC risk independent of static metabolic risk factors—suggests importance of longitudinal phenotyping. | [29] |
HCC: hepatocellular carcinoma; MASLD: Metabolic dysfunction-associated steatotic liver disease; NAFLD: non-alcoholic fatty liver disease; NASH: non-alcoholic steatohepatitis; NA: Non-Alcoholic; MetALD: Metabolic dysfunction-Associated Alcohol-related Liver Disease; PAR: Population Attributable Risk.
Median survival is often less than 12 months, underscoring the importantce to monitor people, especially those at higher risk, such as those with cirrhosis or chronic HBV infection. Because of this, the latest guidelines from the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver recommend getting liver ultrasounds every six months, sometimes combined with alpha-fetoprotein tests. Even though there is no level I evidence supporting this approach, many observational studies have shown that regular monitoring works well for people with cirrhosis. Also, randomized controlled trials have confirmed that surveillance is helpful for those with HBV [30].
Clinical implications for cancer
One of the biggest causes of cancer-related death around the world is still HCC, particularly among individuals with cirrhosis. Improving clinical outcomes requires routine surveillance because it makes early tumor diagnosis possible, which is necessary for access to potentially curative treatments such as radiofrequency ablation, liver transplantation, and surgical resection. An extensive meta-analysis that included 47 studies and more than 15,000 patients showed that surveillance greatly raises the chances of finding HCC early (odds ratio (OR) = 2.08) and getting treatment for it (OR = 2.24). Crucially, even after correcting for lead-time bias, patients who received routine surveillance also had improved overall survival (OR = 1.90). The difference in prognosis is remarkable: 5-year survival rates for early-stage HCC treated with curative intent can reach 70%, while advanced-stage disease usually has a median.
Therapeutic approaches
Therapeutic approaches for MASLD are evolving rapidly, with some of the current approaches involving modification of metabolic risk factors, new pharmacotherapy approaches, and intervention studies targeting risk factors implicated in the progression of disease [31]. As research progresses into the MASLD metabolic, inflammatory, and fibrotic mechanisms, the therapeutic options available to manage MASLD continue to evolve. Current strategies include lifestyle modification, metabolic options, and most current work in pharmacological, molecular, and/or nano-technology therapeutics. The goal of these interventions is to reduce steatosis and inflammation, and halt the fibrosis and progression of long-term disease.
Anti-inflammatory drugs
Inflammation represents a critical driver of MASLD-related hepatocarcinogenesis; thus, anti-inflammatory drugs may act as promising agents to block the development of HCC. Saroglitazar, a dual (Peroxisome proliferator-activated receptors) PPAR-α/γ agonist, has been shown to inhibit tumor development in a NASH-driven HCC mouse model via the reduction of markers of liver injury and pro-inflammatory cytokines such as TNF-α [32]. Similarly, scoparone, a naturally-occurring coumarin derivative, inhibited HCC development in NAFLD mice by inhibiting inflammation-related (p38 Mitogen-Activated Protein Kinase/Also known as Protein Kinase B/Nuclear Factor kappa-light-chain-enhancer of activated B cells) p38-MAPK/Akt/NF-κB signaling pathways. Metformin, the famous licensed antidiabetic drug, has also chemopreventive impacts, as it decreases the incidence of HCC in preclinical models by regulating the immune cell populations and inhibiting inflammatory–metabolic pathways [33].
Antioxidants
Oxidative stress heightens the risk of liver injury and hastens progression from NASH to HCC. Antioxidants are capable of suppressing oxidative stress. Curcumin has been shown to reduce hepatic steatosis and fibrosis in a NASH-HCC mouse model, while downregulating pro-inflammatory cytokines and blocking the (high mobility group box 1 protein) HMGB1/NF-κB translocation, thus suppressing the carcinogenesis process [34]. Additionally, meta-analyses of animal models have further demonstrated that curcumin downregulates Interleukin-6 (IL-6), TNF-α, and other inflammatory markers through multiple signaling pathways (e.g., (Toll-like receptor 4) TLR4/NF-κB, (Kelch-like ECH-associated protein 1 nuclear factor erythroid 2) Keap1/Nrf2), thereby attenuating the progression of NAFLD to HCC [35]. Lycopene, a natural carotenoid of tomatoes, also protects against NASH by attenuating inflammasome activation (NLRP3), NF-κB activation, and by restoring the antioxidant defenses, potentially lowering the risk of HCC [36].
Anti-fibrotic
In MASLD, fibrosis creates an environment that promotes cancer, and anti-fibrotic agents may have the potential to mitigate cancer progression. Pioglitazone, a selective agonist of PPAR-γ, is widely known for its anti-fibrotic properties demonstrated in NASH models, which may reduce fibrosis by modulating multiple signaling pathways such as AMP-activated protein kinase (AMPK) and Mitogen-activated protein kinases (MAPK) that are involved in fibrosis, thereby preventing the fibrotic substrate to HCC. The drug NV556 (a new anti-fibrotic being tested in phase 1 trials) is little studied in HCC, but its capacity to blunt fibrogenic signaling elevates its potential in chemoprevention in fibrotic livers [37].
Lipid metabolism
Disordered lipid metabolism and lipotoxicity contribute to liver injury and carcinogenesis. Interventions with n-3 polyunsaturated fatty acids (PUFAs) can restore lipid homeostasis by decreasing lipotoxic intermediates, which, in turn, can limit hepatocyte stress and possibly promote tumor growth. Bioactive plant-derived supplements, such as mulberry leaf powder, can also modulate lipid metabolism, reduce fatty acid overload, and intervene in lipotoxicity which would lead to reduced inflammation and tumorigenesis [38].
Immunomodulatory
Immune dysregulation in MASLD leads to a tumor-permissive microenvironment. Therapies such as losartan may enhance anti-tumor immunity through reductions in fibrosis. Additionally, beneficial microbes, including Akkermansia muciniphila, have been shown to enhance T-cell mediated responses and improve immunotherapy responses in preclinical models, and thereby re-establish immune monitoring and limit tumor growth [39].
Emerging research and future directions
Flavonoids have proven to be synergistic with traditional chemotherapeutic agents to improve drug effectiveness and to target drug resistance. For example, quercetin has been shown to improve the anticancer ability of 5-fluorouracil and docetaxel, and epigallocatechin gallate (EGCG) improves the cytotoxicity of doxorubicin and gemcitabine. These combinations can lead to improved treatment outcomes while allowing dose reduction to minimize side effects. Recent studies have verified that targeting the ferroptotic pathway may impede the advancement of MASLD. Drugs like the thiazolidinediones (pioglitazone), Glucagon-like peptide-1 (GLP-1) receptors agonists (liraglutide), and a myriad of nutraceuticals including vitamin E, curcumin, quercetin have been found to have examples of anti-ferroptotic activity. These agents have been utilized to target the ferroptotic process through different mechanisms, including inhibitors of acyl-CoA synthetase long-chain family member 4 (ACSL4), activators of glutathione peroxidase 4 (GPX4), and/or stimulators of the Nrf2 antioxidant system. Their ability to modify iron homeostasis, inhibit oxidative stress-related damage, and to inhibit lipid peroxidation validates their influence as broad-spectrum treatment options for target MASLD.
In the future, perhaps our treatment response exploration will include ferroptosis-related biomarkers as a part of clinical trials. It is also important to gain a better understanding of the molecular processes, especially surrounding Factory X Racewear (FXR), AMPK, and mitochondrial factors. It may be possible to find novel treatment targets by identifying ferroptosis modulators in hepatic and extrahepatic tissues (such as adipose tissue and pancreatic β-cells). Additional clinical benefits may be provided by combination treatments that target inflammation, lipid metabolic abnormalities, and iron dysregulation. The application of AI-driven drug discovery techniques and delivery methods based on nanotechnology has the potential to speed up the creation of optimal medicines that target ferroptosis [40]. However, one of the main challenges with ferroptosis-based therapies is that most of the evidence comes from preclinical studies (animal or cell models), and the best options for precisely regulating ferroptosis across the different stages of NAFLD are not well understood, which limits the translation of preclinical studies to human studies [41]. Similarly, in AI-based therapeutic (or prognostic) approaches to liver disease (including MASLD), the hurdles included small and not representative datasets, not externally validated, algorithm transparency, and data integration and privacy issues, all of which limit real-world clinical use [42]. Nonetheless, predictive medicine is changing quickly due to AI and machine learning (ML), especially in detecting high-risk MASLD patients who could develop HCC. Early and precise risk stratification is crucial because MASLD can develop into HCC without obvious clinical symptoms, particularly when severe fibrosis or cirrhosis is not present. Conventional screening methods frequently fail to identify at-risk people in these early, asymptomatic phases. A solution is provided by ML-based models, which use a variety of clinical and laboratory factors to produce individualized risk assessments. A recent study utilizing data from UC Davis and UC San Francisco developed a predictive model for HCC in patients with MASLD, achieving remarkable accuracy of 92.06% and an AUC of 0.97. Among the various clinical variables, the Fibrosis-4 (FIB-4) score emerged as the most influential predictor, followed by bilirubin, alkaline phosphatase (ALP), total cholesterol, and the presence of hypertension. The research underscored the power of ensemble learning algorithms like random forests and gradient boosting to handle complicated, nonlinear medical data, superior to other methods.
Future enhancements will come from integrating predictive systems with heterogeneous data sets; for example, in the future, predictive systems will utilize genomic data, imaging studies, environmental exposures, and lifestyle variables to perform risk stratification. Robust validation in real-world clinical practices and in ethnically diverse populations will be needed. Incorporation of these AI-based models into electronic medical record (EMR) systems could provide real-time risk stratification and inform population-level screening as well as tailored recommendations for individual patients [43].
Conclusion
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease, has become recognized as an important global health problem because of its strong relationship with hepatocellular carcinoma (HCC). MASLD is mainly induced by the triad of obesity, type 2 diabetes, and physical inactivity, ranging from simple steatosis to NASH continuing through to fibrosis, cirrhosis, and liver cancer. One of the important clinical obstacles is that MASLD-associated HCC often develops in non-cirrhotic livers, making early-stage detection particularly difficult. This disease is developed by multifactorial mechanisms, such as insulin resistance, lipid accumulation, oxidative stress, mitochondrial dysfunction, and chronic inflammatory response. Recent advances in transcriptional and post-transcriptional processes have strengthened current understanding of carcinogenic pathways, with the participation of miR-33 and IFI16 splice variants. Non-invasive diagnostic approaches, including liquid biopsies, next-generation sequencing (NGS), and AI-based risk prediction approaches, are becoming increasingly established tools for early detection as well as personalized surveillance. Therapeutic approaches are developing, with particular focus on ameliorating oxidative stress, fibrosis, inflammatory pathways, and lipid dysregulation, as well as targeting bioactive flavonoids, repurposed drugs (i.e., metformin and statins), and delivery systems in the form of nanotechnology. In conclusion, the treatment of MASLD and its oncogenic risks needs a precision-medicine strategy combining dietary and lifestyle interventions, targeted anti-pharmacotherapy, as well as an innovative diagnostic tool.
Availability of data and materials
Not applicable. This review did not generate or analyze any novel data. All information addressed is obtained as a result of published literature referred to in the article in the past.
Author contributions
AK—conceived and designed the review and developed the literature search, data extraction, and analysis. AKS—offered critical advice and helped with literature analysis as well as interpretation of results; helped in editorial modifications, read and endorsed the final manuscript. AK and AKS—initially wrote and edited the manuscript. Both authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Acknowledgment
We would like to acknowledge the Department of Medical Lab Technology, Chandigarh University, for providing the required facilities.
Funding
This research received no external funding.
Conflict of interest
The authors declare no conflict of interest.
REFERENCES
1. Kalligeros M, Henry L, Younossi ZM. Metabolic dysfunction-associated steatotic liver disease and its link to cancer. Metabolism. 2024; 160: 156004.
2. Xue R, Fan JG. Brief introduction of an international expert consensus statement: a new definition of metabolic associated fatty liver disease. Journal of Clinical Hepatology. 2020; 36: 1224–1227. (In Chinese)
3. Estes C, Anstee QM, Arias-Loste MT, Bantel H, Bellentani S, Caballeria J, et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. Journal of Hepatology. 2018; 69: 896–904.
4. Wong RJ. Epidemiology of metabolic dysfunction-associated steatotic liver disease (MASLD) and alcohol-related liver disease (ALD). Metabolism and Target Organ Damage. 2024; 4: 35.
5. Bueverov AO, Bogomolov PO. Nonalcoholic fatty liver disease without obesity: the problem to be solved. Terapevticheskiĭ Arkhiv. 2017; 89: 226–232. (In Russian)
6. Farrell GC, van Rooyen D, Gan L, Chitturi S. NASH is an inflammatory disorder: pathogenic, prognostic and therapeutic implications. Gut and Liver. 2012; 6: 149–171.
7. Liu Z, Lin C, Suo C, Zhao R, Jin L, Zhang T, et al. Metabolic dysfunction–associated fatty liver disease and the risk of 24 specific cancers. Metabolism. 2022; 127: 154955.
8. Vaz K, Clayton-Chubb D, Majeed A, Lubel J, Simmons D, Kemp W, et al. Current understanding and future perspectives on the impact of changing NAFLD to MAFLD on global epidemiology and clinical outcomes. Hepatology International. 2023; 17: 1082–1097.
9. Crane H, Gofton C, Sharma A, George J. MAFLD: an optimal framework for understanding liver cancer phenotypes. Journal of Gastroenterology. 2023; 58: 947–964.
10. Ludwig J, Viggiano TR, McGill DB, Oh BJ. Nonalcoholic steatohepatitis mayo clinic experiences with a hitherto unnamed disease. Mayo Clinic Proceedings. 1980; 55: 434–438.
11. Han SK, Baik SK, Kim MY. Non-alcoholic fatty liver disease: definition and subtypes. Clinical and Molecular Hepatology. 2023; 29: S5–S16.
12. Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, et al.; NAFLD Nomenclature Consensus Group. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023; 78: 1966–1986.
13. Miller DM, McCauley KF, Dunham-Snary KJ. Metabolic dysfunction-associated steatotic liver disease (MASLD): mechanisms, clinical implications and therapeutic advances. Endocrinology, Diabetes & Metabolism. 2025; 8: e70132.
14. Berlanga A, Guiu-Jurado E, Porras JA, Auguet T. Molecular pathways in non-alcoholic fatty liver disease. Clinical and Experimental Gastroenterology. 2014; 7: 221–239.
15. Buzzetti E, Pinzani M, Tsochatzis EA. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism. 2016; 65: 1038–1048.
16. Yagüe-Caballero C, Casas-Deza D, Pascual-Oliver A, Espina-Cadena S, Arbones-Mainar JM, Bernal-Monterde V. MASLD-related hepatocarcinoma: special features and challenges. Journal of Clinical Medicine. 2024; 13: 4657.
17. Qureshi K, Abrams GA. Metabolic liver disease of obesity and role of adipose tissue in the pathogenesis of nonalcoholic fatty liver disease. World Journal of Gastroenterology. 2007; 13: 3540–3553.
18. Maldonado-Rojas ADC, Zuarth-Vázquez JM, Uribe M, Barbero-Becerra VJ. Insulin resistance and Metabolic dysfunction-associated steatotic liver disease (MASLD): pathways of action of hypoglycemic agents. Annals of Hepatology. 2024; 29: 101182.
19. Phoolchund AGS, Khakoo SI. MASLD and the development of HCC: pathogenesis and therapeutic challenges. Cancers. 2024; 16: 259.
20. Mazzolini G, Sowa JP, Atorrasagasti C, Kücükoglu Ö, Syn WK, Canbay A. Significance of simple steatosis: an update on the clinical and molecular evidence. Cells. 2020; 9: 2458.
21. Vaz J, Jepsen P, Strömberg U, Midlöv P, Eriksson B, Buchebner D, et al. Metabolic dysfunction-associated steatotic liver disease has become the most common cause of hepatocellular carcinoma in Sweden: a nationwide cohort study. International Journal of Cancer. 2025; 156: 40–51.
22. Fernández-Tussy P, Cardelo MP, Zhang H, Sun J, Price NL, Boutagy NE, et al. MiR-33 deletion in hepatocytes attenuates MASLD-MASH-HCC progression. JCI Insight. 2024; 9: e168476.
23. Vitellius C, Desjonqueres E, Lequoy M, Amaddeo G, Fouchard I, N’Kontchou G, et al. MASLD-related HCC: multicenter study comparing patients with and without cirrhosis. JHEP Reports. 2024; 6: 101160.
24. Ebrahimi F, Hagström H, Sun J, Bergman D, Shang Y, Yang W, et al. Familial coaggregation of MASLD with hepatocellular carcinoma and adverse liver outcomes: nationwide multigenerational cohort study. Journal of Hepatology. 2023; 79: 1374–1384.
25. Shinde S, Bigogno CM, Simmons A, Kathuria N, Ghose A, Apte V, et al. Precision oncology through next generation sequencing in hepatocellular carcinoma. Heliyon. 2025; 11: e42054.
26. Rodriguez LA, Schmittdiel JA, Liu L, Macdonald BA, Balasubramanian S, Chai KP, et al. Hepatocellular carcinoma in metabolic dysfunction-associated steatotic liver disease. JAMA Network Open. 2024; 7: e2421019.
27. Peng Y, Wang P, Liu F, Wang X, Si C, Gong J, et al. Metabolic dysfunction-associated steatotic liver disease and cancer risk: a cohort study. Diabetes, Obesity and Metabolism. 2025; 27: 1940–1949.
28. Petrelli F, Manara M, Colombo S, De Santi G, Ghidini M, Mariani M, et al. Hepatocellular carcinoma in patients with nonalcoholic fatty liver disease: a systematic review and meta-analysis. Neoplasia. 2022; 30: 100809.
29. Jeong S, Oh YH, Ahn JC, Choi S, Park SJ, Kim HJ, et al. Evolutionary changes in metabolic dysfunction-associated steatotic liver disease and risk of hepatocellular carcinoma: a nationwide cohort study. Clinical and Molecular Hepatology. 2024; 30: 487–499.
30. Singal AG, Pillai A, Tiro J. Early detection, curative treatment, and survival rates for hepatocellular carcinoma surveillance in patients with cirrhosis: a meta-analysis. PLOS Medicine. 2014; 11: e1001624.
31. Drygalski K. Pharmacological treatment of MASLD: contemporary treatment and future perspectives. International Journal of Molecular Sciences. 2025; 26: 6518.
32. Giri SR, Bhoi B, Trivedi C, Rath A, Rathod R, Sharma A, et al. Saroglitazar suppresses the hepatocellular carcinoma induced by intraperitoneal injection of diethylnitrosamine in C57BL/6 mice fed on choline deficient, l-amino acid- defined, high-fat diet. BMC Cancer. 2023; 23: 59.
33. Zhang Y, Wang H, Xiao H. Metformin actions on the liver: protection mechanisms emerging in hepatocytes and immune cells against NASH-related HCC. International Journal of Molecular Sciences. 2021; 22: 5016.
34. Afrin R, Arumugam S, Rahman A, Wahed MI, Karuppagounder V, Harima M, et al. Curcumin ameliorates liver damage and progression of NASH in NASH-HCC mouse model possibly by modulating HMGB1-NF-κB translocation. International Immunopharmacology. 2017; 44: 174–182.
35. Li Y, Deng X, Tan X, Li Q, Yu Z, Wu W, et al. Protective role of curcumin in disease progression from non-alcoholic fatty liver disease to hepatocellular carcinoma: a meta-analysis. Frontiers in Pharmacology. 2024; 15: 1343193.
36. Gao X, Zhao X, Liu M, Zhao H, Sun Y. Lycopene prevents non-alcoholic fatty liver disease through regulating hepatic NF-κB/NLRP3 inflammasome pathway and intestinal microbiota in mice fed with high-fat and high-fructose diet. Frontiers in Nutrition. 2023; 10: 1120254.
37. Ni XX, Li XY, Wang Q, Hua J. Regulation of peroxisome proliferator-activated receptor-gamma activity affects the hepatic stellate cell activation and the progression of NASH via TGF-β1/Smad signaling pathway. Journal of Physiology and Biochemistry. 2021; 77: 35–45.
38. Jump DB, Depner CM, Tripathy S, Lytle KA. Potential for dietary ω-3 fatty acids to prevent nonalcoholic fatty liver disease and reduce the risk of primary liver cancer. Advances in Nutrition. 2015; 6: 694–702.
39. Gu L, Zhu Y, Lee M, Nguyen A, Ryujin NT, Huang JY, et al. Angiotensin II receptor inhibition ameliorates liver fibrosis and enhances hepatocellular carcinoma infiltration by effector T cells. Proceedings of the National Academy of Sciences. 2023; 120: e2300706120.
40. Zhu B, Wei Y, Zhang M, Yang S, Tong R, Li W, et al. Metabolic dysfunction-associated steatotic liver disease: ferroptosis related mechanisms and potential drugs. Frontiers in Pharmacology. 2023; 14: 1286449.
41. Zhou X, Fu Y, Liu W, Mu Y, Zhang H, Chen J, et al. Ferroptosis in chronic liver diseases: opportunities and challenges. Frontiers in Molecular Biosciences. 2022; 9: 928321.
42. Žigutytė L, Sorz-Nechay T, Clusmann J, Kather JN. Use of artificial intelligence for liver diseases: a survey from the EASL congress 2024. JHEP Reports. 2024; 6: 101209.
43. Sarkar S, Alurwar A, Ly C, Piao C, Donde R, Wang CJ, et al. A machine learning model to predict risk for hepatocellular carcinoma in patients with metabolic dysfunction-associated steatotic liver disease. Gastro Hep Advances. 2024; 3: 498–505.