
Download
Original Articles Nephrology
Clinicopathological Features of Lupus Nephritis Patients in North-East India; A Single Center Retrospective Observational Study
Shahzad Alam1, Manzoor Parry2*, Manjuri Sharma1, Hamad Jeelani1, Mastakim Mazumder1
1Department of Nephrology, Gauhati Medical College and Hospital,•Guwahati, India;
2Department of Nephrology, Sher I Kashmir Institute of Medical Sciences Srinagar, Srinagar, India
Abstract
Clinicopathological presentation of lupus nephritis (LN) patients varies with different race and ethinicity of the population. Only few studies describe clinicopathological spectrum of LN patients in the Indian population. The aim of this study was to determine the clinicopathological spectrum of LN in the North-East Indian population. This was a retrospective observational study that included patients with LN at a tertiary care center in North-East India from March 2007 to August 2018. Clinical and histopathological data at the time of presentation were collected from hospital records. Renal biopsies were examined by light microscopy and direct immunofluorescence techniques. A total of 340 patients of LN were included in this study. The mean age of presentation was 22.42 ± 4.3 years. The minimum age at presentation was 8 years and 18.8% belonged to the <18 year age group. The present study showed a male:female ratio of 1:8. The majority of patients were of class IV (71.9%). Arthralgia (47.1%) and anemia (60.3%) were the most common presenting symptom and sign, respectively. Immunoglobulin (Ig) G was the most abundant immunoglobulin (positive in 98.47%) and the least positive was IgA (positive in 41.18%). Complement (C) 3 and C1q were positive in all. Full house deposition was found in 59.3% of the biopsies. The rates of hypertension, microscopic hematuria, renal dysfunction, and nephrotic syndrome were 43.5, 59.12, 45.9, and 35.3%, respectively. Patients of LN in the North-East Indian population present at an earlier age with a more severe form of the disease (class IV) at the time of presentation.
Key words: clinicopathological presentation, histopathology, lupus nephritis, systemic lupus erythematosus
Received: 30 September 2021; Accepted after Revision: 3 November 2021; Published: 10 December 2021
Author for correspondence: Manzoor Parry, Department of Nephrology, Sher I Kashmir Institute of Medical Sciences Srinagar, Srinagar, India. Email: maparry33@gmail.com
How to cite: Alam S, et al. Clinicopathological Features of Lupus Nephritis Patients in North-East India; A Single Center Retrospective Observational Study. J Ren Hepat Disord. 2021 6(1):1–6.
Doi: http://dx.doi.org/10.15586/jrenhep.v6i1.130
Copyright: Alam S, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
Lupus nephritis (LN) is one of the most important and severe complications of systemic lupus erythematosus (SLE) (1). In the SLE population, 40–70% of the patients develop LN in their natural clinical course of the disease (2). Kidney biopsies play an important role in the diagnosis, management, and prognosis of patients with LN. There is generally a good correlation between the morphological lesions and clinicolaboratory features; however, this might vary in some cases (3). Hence, kidney biopsies are essential to accurately determine the extent of parenchymal damage in LN and to guide treatment. Despite the advancement in the therapy of lupus, conversion rate to end-stage renal disease (ESRD) has remained around 10% in 5–10 years of disease course, which has remained unchanged over the last 3 decades (4, 5).
The prevalence of LN is higher in Indo-Asians (Asians of the Indian subcontinent) in comparison to the white population, although long-standing prognosis is similar in both populations (6, 7). So, race is also an important factor to predict severity and outcome in LN. Presently, only a few studies are available which throw light on the exact clinicopathological spectrum in LN patients in the Indian population.
Materials and Methods
This was a retrospective observational study done in the Department of Nephrology, Gauhati Medical College and Hospital Assam, a tertiary referral center for the whole of the North-Eastern part of India. In this study, we aimed to conduct a retrospective analysis of the clinico-pathological features of biopsy-proven LN patients. The patients fulfilled the revised American College of Rheumatology (ACR) criteria for SLE (8). LN cases confirmed through renal biopsy were classified according to the 2003 ISN/RPS LN classification (9).
The study was conducted from March 2007 to August 2018. All performed renal biopsies were sent to a reference laboratory and reviewed by the same nephropathologist. Patients with renal biopsy having more than 10 glomerli were included in this study. Patients with uncontrolled disease in any organ system not related to SLE or LN, concomitant chronic conditions requiring immune-suppressive treatment, history of renal or any other organ transplant, viral ( like hepatitis B, hepatitis C, human immunodeficiency virus) infection, and those who did not provide consent were excluded.
Light microscopy and direct immunofluorescence techniques were used to examine the renal biopsy tissues. For light microscopy, biopsy specimens were fixed in 4.5% buffered formaldehyde (4.5%). Stains employed in examination included periodic acid-schiff, hematoxylin and eosin, Masson’s trichrome, and silver methenamine. Pathological parameters in light microscopy examination, such as activity indexes (AI) and chronicity indexes (CI), were assessed by renal histopathologists by using a semiquantitative scoring system of specific biopsy features (10, 11).
The immunofluorescence intensity of immunoglobulin IgG, IgA, IgM, complement 3 (C3), and complement 1q (C1q) deposition were graded semiquantitatively from 0 to 4+. Electron microscopy examination was not done.
Detailed clinical data of each patient were thoroughly analyzed retrospectively. Informed consent was taken from the patients using contact numbers retrieved from hospital records. Approval from the Ethics Committee of GMCH (with the ethics code of MC/190/2018/Pi-I/145), Assam, India, was taken. Baseline clinical examination included serum anti-ds DNA antibodies, anti-neutrophil antibody (ANA), hemoglobin (Hb), red blood cell count, total white blood cell count (TLC), platelet count, serum albumin, serum creatinine (S.Cr), complement 3(C3), complement 4 (C4), urine routine microscopy, and 24-h urine protein.
Statistical analysis
Statistical software, Statistical Package for the Social Sciences (SPSS version 22.0), was used to analyze relevant data. Categorical data were presented in the form of numbers and percentages. Continuous data were expressed as mean ± standard deviation (SD).
Results
A total of 340 patients of LN were included in this study. Among all of the included 340 LN patients diagnosed during this duration in the Department of Nephrology GMCH Guwahati Assam, 301 (88.53%) were females and 39 (11.47%) were males (Figure 1). The male to female ratio was 1:8 and the average age was 22.42 ± 4.3 years at the time of presentation. The minimum age at presentation was 8 years and 64 patients (18.8%) belonged to the <18 year age group.
Figure 1: Gender distribution of the study population.
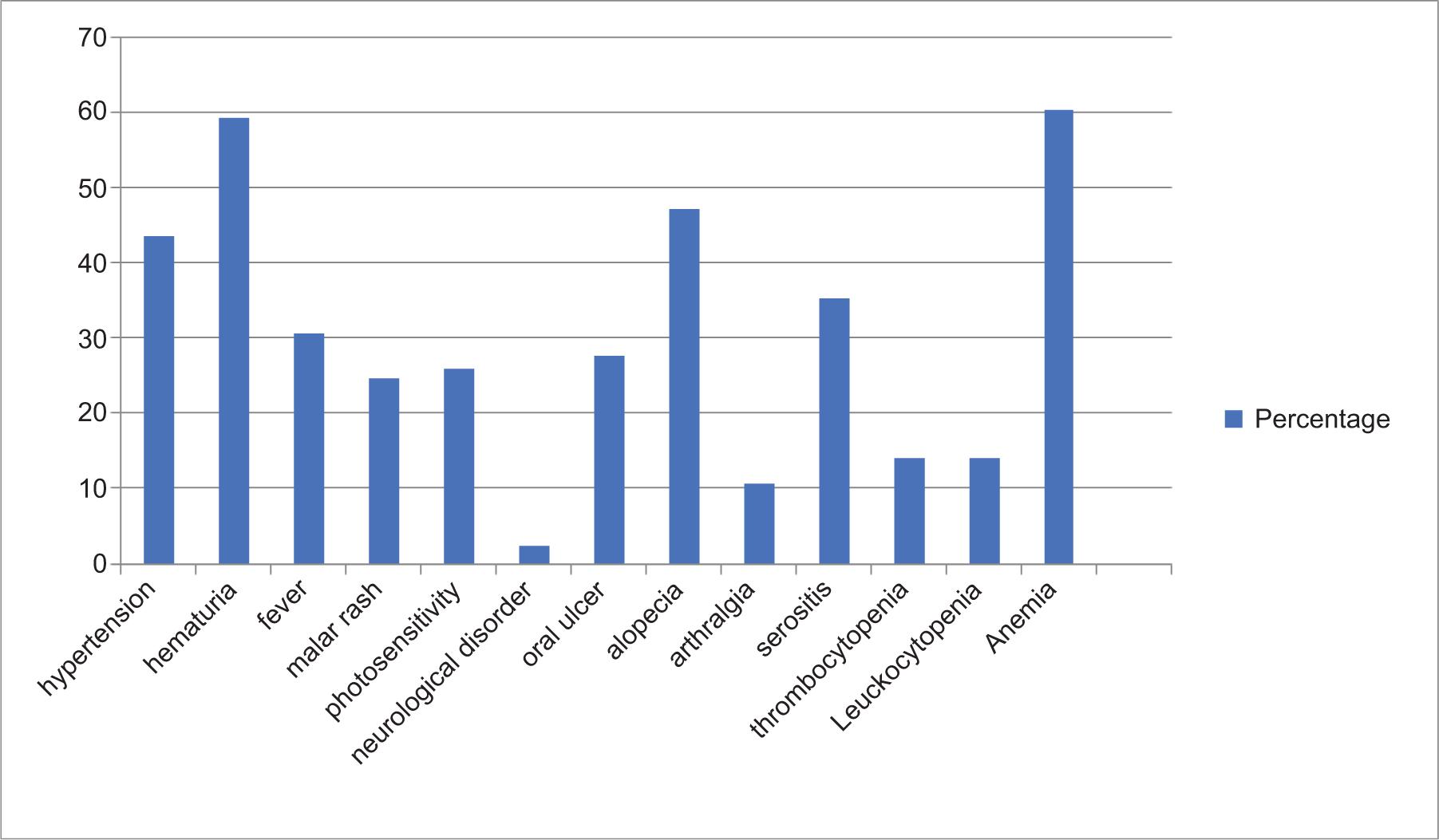
Hypertension was found in 148 (43.5%) patients, and their mean systolic and diastolic blood pressures were 139.38 ± 15.86 mm Hg and 83.6 ± 8.24 mm Hg, respectively. The most common clinical symptom at the time of presentation was arthralgia seen in 47.1% (n = 160) of the patients. Anemia was the most common presenting sign, seen in 60.3% (n = 205) of the patients. Regarding other clinical presentations, fever was present in 30.6% (n = 104) patients, malar rash in 24.7% (n = 84) patients, photosensitivity in 25.9% (n = 88) patients, oral ulcer in 24.7% (n = 84) patients, alopecia in 18.8% (n = 64) patients, serositis in 10.6% (n = 36) patients, thrombocytopenia in 14.1% (n = 48) patients, and leukocytopenia in 14.1% (n = 48) patients. Neurological disorder (2.4%) was the least common clinical presentation in LN patients (Table 1 and Figure 2).
Table 1: Clinical features of our study population (in percentage).
| Clinical & lab parameters | Number of patients | Percentage |
|---|---|---|
| Hypertension | 148 | 43.5 |
| Hematuria | 201 | 59.11 |
| Fever | 104 | 30.6 |
| Malar rash | 84 | 24.7 |
| Photosensitivity | 88 | 25.9 |
| Neurological disorder | 8 | 2.4 |
| Oral ulcer | 84 | 24.7 |
| Alopecia | 64 | 18.8 |
| Arthralgia | 160 | 47.1 |
| Serositis | 36 | 10.6 |
| Nephrotic syndrome | 120 | 35.3 |
| Acute kidney injury | 156 | 45.9 |
| Thrombocytopenia | 48 | 14.1 |
| Leukocytopenia | 48 | 14.1 |
| Anemia | 205 | 60.3 |
Figure 2: Clinical features of lupus nephritis patients at the time of presentation.
Hematuria was found in 59.12% (n = 201) patients. Among the 340 patients, 35.3% (n = 120) fulfilled the definition of nephrotic syndrome, and 45.9 % (n = 156) patients were admitted with renal dysfunction. The mean values of hemoglobin, serum creatinine, serum albumin, and 24-h urinary protein were 11.12 ± 0.09 g/dL, 2.28 ± 0.045 mg/dL, 2.32 ± 0.032 g/dL, and 2.22 ± 0.122 g/day at the time of presentation, respectively. Mean titer of serum ANA and Anti-dsDNA were 2.17 ± 0.48 and 2.20 ± 0.46, respectively (Table 2).
Table 2: Clinical and lab parameters of lupus nephritis patients at the time of presentation.
| Clinical and lab parameters | Mean ± SD | Range |
|---|---|---|
| No. of patients = 340 | ||
| Gender (M/F) = 39/301 (1:7.72) | ||
| Age (years) | 22.42 ± 14 | 8–37 |
| Hb (g%) | 11.12 ± 0.09 | 8.7–13.8 |
| S.Cr (mg/dL) | 2.28 ± 0.05 | 0.8–4.8 |
| Serum Albumin (g/dL) | 2.32 ± 0.03 | 0.9–3.1 |
| 24 h Urine protein (g/day) | 2.22 ± 0.12 | 0.50–12.4 |
| ANA (0–4 + semiquantitative scale) | 2.17 ± 0.48 | 0–3.0 |
| Anti-ds DNA (0–4 + semiquantitative scale) | 2.20 ± 0.46 | 0–3.0 |
| SBP (mm-Hg) | 139.38 ± 15.86 | 120–170 |
| DBP(mm-Hg) | 83.6 ± 8.24 | 66–96 |
Hb: Hemoglobin; S.Cr: Serum creatinine; ANA: anti-nuclear antibody; ds DNA: Double-stranded deoxyribonucleic acid; SBP: systolic blood pressure; DBP: Diastolic blood pressure.
Table 3: Frequency distribution of patients according to ISN/RPS classification of lupus nephritis.
| Biopsy | ||
|---|---|---|
| No. of biopsies | 340 | |
| No. of glomeruli | 17.47 ± 2.82 | 11–24 |
| Class | Frequency | Percent |
| II | 28 | 8.2 |
| V | 20 | 5.9 |
| VI | 8 | 2.4 |
| III | 36 | 10.6 |
| V–III | 4 | 1.2 |
| IV–S | 48 | 14.2 |
| IV–G | 168 | 49.4 |
| V–IV | 28 | 8.3 |
II: Class two; III: Class three; IV: Class four; V: Class five; S: segmental; G: Global.
Table 4: Microscopic characteristics of renal biopsy in LN patients.
| Light microscopy | Mean | Range |
|---|---|---|
| AI score | 7.28 ± 3.22 | 0–13 |
| Cellular crescents | 1.25 ±1.36 | 0–6 |
| Karyorrhexis/fibrinoid necrosis | 1.05 ± 0.55 | 0–6 |
| Interstitial inflammation | 1.22 ± 0.56 | 0–3 |
| Glomerular leukocyte | 1.21 ± 0.738 | 0–3 |
| Endocapillary hypercellularity | 1.15 ± 0.64 | 0–3 |
| Subendothelial immune deposition | 1.34 ± 0.68 | 0–3 |
| CI score | 3.79 ± 1.58 | 0–9 |
| Fibrous crescents | 0.59 ± 0.0.49 | 0–3 |
| Tubular atrophy | 0.95 ± 0.37 | 0–3 |
| Interstitial fibrosis | 0.97 ± 0.41 | 0–3 |
| Glomerular sclerosis | 1.31 ± 0.47 | 0–3 |
| Immunofluorescence parameters | ||
| IgG | 2.13 .± 0.59 | 0–3 |
| Ig M | 1.92 ± 0.382 | 0–2 |
| Ig A | 0.41 ± 0.63 | 0–1 |
| C1 q | 1.60 ± 0.49 | 1–2 |
| C3 | 1.98 ± 0.12 | 1–2 |
AI: Activity index; CI: Chronicity index; Ig: Immunoglobulins; C1q: Complement 1q; C3: Complement 3.
On histopathological evaluation, the number of average glomeruli per biopsy was 17.47 ± 2.82. Pursuant to light microscopy features, patients were classified into different classes. Class IV was the most common morphological pattern (63.6%) with 49.4% having class IV-G and 14.2% having class IV-S. Class III was seen in 10.6%.
In light microscopy, the average AI was 7.28 ± 3.22 and average CI was 3.79 ± 1.58. The semiquantitative scale average cellular crescent score was 1.25 ± 1.36, average karyorrhexis/fibrinoid necrosis score was 1.05 ± 0.55, and average interstitial inflammation score was 1.22 ± 0.56. Glomerular leukocytosis score was 1.21% ± 0.74, average endocapillary hypercellularity score was 1.15 ± 0.64, and average subendothelial immune deposition score was 1.34 ± 0.68.
In CI, average fibrous crescent score was 0.59 ± 0.49, average tubular atrophy score was 0.95 ± 0.37, average interstitial fibrosis score was 0.97 ± 0.41, and average glomerular sclerosis score was 1.31 ± 0.47.
Immunofluorescence parameters on semiquantitative scale average IgG score was 2.13 ± 0.59, average IgM score was 1.98 ± 0.38, average IgA score was 0.41 ± 0.63, average C3 score was 1.98 ± 0.12, and average C1q score was 1.60 ± 0.49. Full house immune deposition was found in 41.18%. In the IF study, IgG was most abundant and found positive in 98.47% (n = 328) and least positive was IgA which was positive in 41.18% (n = 140). C3 and C1q were positive in all patients.
Discussion
LN is a common and the most debilitating complication of SLE and can present with any type of glomerular injury (12). This study was carried out to examine the clinicopathological characteristics of LN among North-East Indian patients. It is crucial to investigate whether evidence of nephropathy is present or not in patients with SLE since patients with renal involvement have a far poor prognosis than those without renal pathology (13).
The study included adults as well as children. Mean age at the time of presentation was 22.42 ± 4.3 years. Minimum age of presentation was 8 years and 64 patients (18.8%) belonged to the <18 year age group. One study from Bangladesh, done in 2006, showed that the mean age of the LN patients was 26 ± 11.97 years (14). Mean age of LN patients were 35.4 years and 33 ± 14 years, respectively, in studies in Singapore and China (15, 16). A study in Iran showed a mean age of 25.6 ± 10.3 years (17) and in other studies, the mean age varied from 33.5 ± 14 years to 36.8 ± 13.8 years (18, 19). Age of presentation of LN patients of our study is similar to patients in Iran and Bangladesh but differs from those in China and Singapore. Our patients with LN present a decade younger than their Chinese counterparts, which may be due to different ethnicity (20).
The present study shows a male to female ratio of 1:8, similar to the studies from UK, Iran, and Bangladesh having a male to female ratio of 1: 8, 1:13, and 1:10, respectively (14, 17, 21). Our study differs from the studies carried out in Singapore and Pakistan showing a male: female ratio of 1:4 and 1:2, respectively (15, 22). This difference could be due to the racial and geographical variation of LN. This establishes the fact that clinical manifestations vary according to the geographic location of the patients with LN (17, 23). More male patients than usual for LN in some studies was explained to some extent by the slight male dominance in reaching the tertiary care center for the same disease than their female counterparts.
In our study, maximum patients were of class IV – 71.9% (n = 244); among them, isolated class IV were 63.6% (n = 216). Class IV-S had 14.2% (n = 48). In a Bangladeshi study, ISN/RPS class IV-G was found to be the most frequent, representing about 64.7% of the total cases, and 11.8% cases were class IV-S patients (14). One Chinese cohort study with 172 patients belonging to ISN/RPS class IV patients found 152 cases in class IV-G and only 20 cases in class IV-S (12). In a pediatric LN study by Shrivastava et al., class IV LN was the most common class (24).
In our study, the most common clinical symptom at the time of presentation was arthralgia (47.1%), and anemia (60.3%) was the most common presenting sign. In Baqui et al.’s study, the most common clinical presentations of the patients at the time of renal biopsy was arthralgia (82.4%) (14).
In immunofluorescence, our study showed 100% cases of any type of glomerular deposits. Regarding immunoglobulins, IgG was most abundant and was positive in 98.47%, and the least positive was IgA (positive in 41.18%). C3 and C1q were positive in all patients. Nossent et al. found that 98.5% of their biopsies showed glomerular deposits and C3 was found to be the most common (93%), followed by IgM (88%), IgA (84%), and IgG (78%) (25). Das et al. also showed C3 deposition in 96.2% cases, followed by IgM in 84.6% cases of patients of LN (26). In Baqui et al.’s study, IgG (85.29%) was the most common immunoglobulin. The next common was C3, which was present in 79.4% of the renal biopsy specimens (14).
In our study, full house immune deposition was found in 41.18% of the biopsies. Das et al. also found a full house pattern of immunoglobulin deposition in 67% of the biopsies (26). Baqui et al.’s study showed full house deposition in 59.3% of the biopsies (14).
Hypertension was found in 43.5% of the patients in our study. Hematuria by urine examination was diagnosed in 59.12% of LN patients in our study. In our study, 35.3% of the patients fulfilled the definition of nephrotic syndrome. Studies on LN patients reported that the prevalence of hypertension, microscopic hematuria, and nephrotic syndrome was 30, 80, and 50%, respectively (27). Almost half (45.9%) of the patients were admitted with kidney dysfunction in our study. In a study by Anne et al. on LN, approximately 40% of the affected individuals developed some degree of renal impairment (28).
Study Limitations
This study has some limitations mainly due to its retrospective design and being a single-center study. Also, electron microscopy was not available at our center, again limiting this study.
Conclusion
This study represents significant data to understand the clinical and morphological presentation of LN in the North-East Indian population. Patients of LN in the North-East Indian population have an earlier age of onset of disease, a more severe form of the disease at the time of presentation (class IV disease). Severe and earlier age of presentation of LN underscores the need for biopsy at the earliest and treating promptly to improve the long-term outcome of LN. Arthralgia and anemia were the most common presenting symptom and sign, respectively. Neurological disorder was the least common clinical presentation.
Disclosure
This is an original work and has not been published elsewhere. The paper has been approved by the authors’ team.
REFERENCES
1. Lorenz G1, Desai J, Anders HJ. Lupus nephritis: update on mechanisms of systemic autoimmunity and kidney immunopathology. Curr Opin Nephrol Hypertens. 2014 May;23(3): 211–7. 10.1097/01.mnh.0000444816.57378.21
2. Kaul A, Gordon C, Crow MK, Touma Z, Urowitz MB, Vollenhoven RV, et al. Systemic lupus erythematosus. Nat Rev Dis Primers. 2016; 2: 16039. doi:10.1038/nrdp.2016.39
3. Tang Y, Zhang W, Zhu M, Zheng L, Xie L, Yao Z, et al. Lupus nephritis pathology prediction with clinical indices. Scientific Reports. 2018 Jul 6;8(1): 1–8. 10.1038/s41598-018-28611-7
4. Croca SC, Rodrigues T, Isenberg DA.: Assessment of a lupus nephritis cohort over a 30-year period. Rheumatology (Oxford). 2011; 50: 1424–1430. 10.1093/rheumatology/ker101
5. Ward MM.: Changes in the incidence of end-stage renal disease due to lupus nephritis in the United States, 1996–2004. J Rheumatol. 2009; 36: 63–67. 10.3899/jrheum.080625
6. Seligman VA, Lum RF, Olson JL, Li H, Criswell LA. Demographic differences in the development of lupus nephritis: Aa retrospective analysis. Am J Med. 2002;112: 726–9. 10.1016/S0002-9343(02)01118-X
7. Chan TM, Tse KC, Tang CS, Lai KN, Li FK. Long-term outcome of patients with diffuse proliferative lupus nephritis treated with prednisolone and oral cyclophosphamide followed by azathioprine. Lupus. 2005;14: 265–72. 10.1191/0961203305lu2081oa
8. Weening JJ, D’Agati VD, Schwartz MM, Seshan SV, Alpers CE, Appel GB, et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. J Am Soc Nephrol. 2004; 15(2): 241–50. 10.1097/01.ASN.0000108969.21691.5D
9. Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematous. Arthritis Rheum. 1997; 40(9): 1725. 10.1002/art.1780400928
10. Hachiya A, Karasawa M, Imaizumi T, Kato N, Katsuno T, Ishimoto T, et al. The ISN/RPS 2016 classification predicts renal prognosis in patients with first-onset class III/IV lupus nephritis. Scientific Reports. 2021 Jan 15;11(1): 1–2. 10.1038/s41598-020-78972-1
11. Austin HA, III, Boumaps DT, Vaughan EM, Balow JE. Predicting renal outcomes in severe lupus nephritis: contributions of clinical and histologic data. Kidney Int. 1994; 45: 544–550. 10.1038/ki.1994.70
12. Yu F, Tan Y, Wu LH, Zhu SN, Liu G, Zhao MH. Class IV-G and IV-S lupus nephritis in Chinese patients: a large cohort study from a single center. Lupus. 2009;18: 1073. 10.1177/0961203309106795
13. Alba V, Lucia S, Cristina C, Giovanni MF, Sandra L, Alessandro NC, et al. Lupus nephritis: the value of biochemical and immunological monitoring of disease activity. Ren Fail. 1996;18: 755–763. 10.3109/08860229609047704
14. Baqui MN, Akhter S, Kabir E, Islam MS. A clinicopathological study on lupus nephritis; experience of 34 cases from Bangladesh. J Nephropharmacol. 2016; 5(1): 19–23.
15. Gun HC, Yoon KH, Fong KY. Clinical outcomes of patients with biopsy-proven lupus nephritis in NUH. Singapore Med J. 2002;43: 614–16.
16. Zheng H, Chen Y, Ao W, Shen Y, Chen X, Dai M, et al. Antiphospholipid antibody profiles in lupus nephritis with glomerular microthrombosis: a prospective study of 124 cases. Arthritis Res Ther. 2009;11(3): 93. 10.1186/ar2736
17. Nezhad ST, Sepaskhah R. Correlation of clinical and pathological findings in patients with lupus nephritis: a five year experience in Iran. Saudi Journal of Kidney Disease and Transplantation. 2008;19: 32–40.
18. Donadio JV, Hart GM, Bergstralh EJ, Holley KE. Prognostic determinants in lupus nephritis: a long-term clinicopathologic study. Lupus. 1995;4: 109–15. 10.1177/096120339500400206
19. Hill GS, Delahousse M, Nochy D, Tomkiewicz E, Rémy P, Mignon F, Gary SH, Michel D, Dominique N, Elizabeth T, Philippe RM, Franc, et al. A new morphologic index for the evaluation of renal biopsies in lupus nephritis. Kidney Int. 2000;58: 1160–73. 10.1046/j.1523-1755.2000.00272.x
20. Ong C, Nicholls K, Becker G. Ethnicity and lupus nephritis: an Australian single centre study. Intern Med J. 2011;41: 270–8. 10.1111/j.1445-5994.2009.02159.x
21. Patel M, Clarke AM, Bruce IN, Symmons D. The prevalence and incidence of biopsy-proven lupus nephritis in the UK: Eevidence of an ethnic gradient. Arthritis Rheum. 2006 Sep; 54(9): 2963–9. 10.1002/art.22079
22. Rabbani MA, Memon GM, Ahmad B, Memon S, Tahir SA, Tahir S. Percutaneous renal biopsy results: a retrospective analysis of 511 consecutive cases. Saudi J Kidney Dis Transpl. 2012 May; 23(3): 614–18.
23. Kosaraju K, Shenoy S, Suchithra U. A cross-sectional hospital based study of autoantibody profile and clinical manifestation of systemic lupus erythematosus in South Indian patients. Indian J Med Microbiol. 2010;28: 245–7. 10.4103/0255-0857.66487
24. Srivastava P, Abujam B, Misra R, Lawrence A, Agarwal V, Aggarwal A. Outcome of lupus nephritis in childhood onset SLE in North and Central India: single-centre experience over 25 years. Lupus. 2016 Apr;25(5): 547–57. 10.1177/0961203315619031
25. Nossent H, Berden J, Swaak T. Renal immunofluorescence and the prediction of renal outcome in patients with proliferative lupus nephritis. Lupus. 2000;9: 504–10. 10.1177/096120330000900705
26. Das R, Saleh A, Kabir A, Talukder SI, Kamal M. Immunofluorescence studies of renal biopsies. Dinajpur Med Col J. 2008;1: 8–13.
27. Salem Almaani S, AlexaMeara A, Brad H. Rovin BH. Update on Llupus Nnephritis. CJASN. May 2017;,12(5): 825–835. 10.2215/CJN.05780616
28. Davidson A. What is damaging the kidney in lupus nephritis?. Nature Reviews Rheumatology. 2016 Mar 12(3): 143–53. 10.1038/nrrheum.2015.159