
Download
Original Articles Nephrology
Clinical Profile and Outcomes of COVID-19 in Renal Transplant Recipients
Mohit Mahajan, Naresh Pahwa, Shraddha Goswami*, Vijay Malviya, Vishnu Shukla, Trishala Chhabra
Department of Nephrology, SAIMS Medical College, Indore, Madhya Pradesh, India
Abstract
There is minimal information on coronavirus disease 2019 (COVID-19) in developing countries regarding renal transplant recipients (RTRs). This paper aimed to study the clinical profile, immunosuppressive regimen, treatment, and outcomes in an RTR with COVID-19. This retrospective study was conducted in the nephrology department of Sri Aurobindo Medical College & Postgraduate Institute, Indore (MP), India, from April 1, 2020 to December 15, 2020. We studied 15 patients, of which 13 were treated at our hospital and two were treated in OPD. The median age of transplant recipients was 45 (Interquartile range [IQR]: 26–62) years, the majority being males, and recipients presented at a median of 4 (IQR: 0.3–11) years after transplant. The most common comorbidities included hypertension in 14 (94%) and diabetes 3 (20%) patients. The presenting symptoms at presentation were cough (80%), headache (52%), fever (46%), and breathlessness (26%). Clinical severity as per computerized tomography (CT) severity score ranged from mild (20%), moderate (53%), and severe (27%). Strategies to modify immunosuppressants included discontinuation of antimetabolites without changes in calcineurin inhibitors and steroids (100%). Antiviral therapy (Favipiravir and Remdesivir) was associated with better outcomes and reduced hospital stay. Risk factors for mortality included ABO-incompatibility, severity of disease, high Coronavirus Disease 2019 (COVID-19) Reporting and Data System (CO-RADS) score, allograft dysfunction before COVID-19 infection, acute kidney injury, elevated inflammatory markers, and intensive care unit/ventilator requirement. Overall patient mortality was 13.2%. Risk factor for mortality in COVID-19 positive with RTR appears to be ABO-incompatible transplant, having a previous history of rejection, and patient requiring ventilatory support.
Key words: acute kidney injury, corona virus disease, intensive care unit, renal transplant recipients, mycophenolate mofetil
Received: 13 October 2021; Accepted after Revision: 7 December 2021; Published: 23 December 2021
Author for correspondence: Dr. Shraddha Goswami, Associate Professor, Nephrology Department, SAIMS University, Indore, Madhya Pradesh 453555, India. Email: shraddhagoswami17@gmail.com
How to cite: Mahajan M, et al. Clinical Profile and Outcomes of COVID-19 in Renal Transplant Recipients. J Ren Hepat Disord. 2021 6(1):10–16.
Doi: http://dx.doi.org/10.15586/jrenhep.v6i1.133
Copyright: Mahajan M, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
In December 2019, the coronavirus (severe acute respiratory syndrome coronavirus; SARS-CoV-2) spread out from a city of Hubei, China, to most of the world (1). On March 11, 2020, the World Health Organization (WHO) announced the coronavirus disease 2019 (COVID-19) as a global pandemic. Transplant recipients were at a higher risk of severe bacterial and viral infections because of diminished T-cell immunity, thereby putting them at a higher risk of infection and mortality from COVID-19. From 2013 to 2018, 49,155 transplants were performed in India, which included 39,000 live and 10,155 cadaver donor transplants. Of these, 38,332 were kidney (live donor = 32,584, cadaver donor = 5748), 9383 were liver (live donor = 6416, cadaver donor = 2967), 895 were heart, 459 were lung, 78 were pancreas, and 8 were small bowel transplants. Based on the 2018 data, India ranks second globally in transplant volume (2). Uptil December 15, 2020, India reported 99,30,741 confirmed COVID-19 positive patients, while city of Indore had 52,660 patients, being highest in the state of Madhya Pradesh (3).
Renal transplant recipients (RTRs) have a higher risk of developing severe COVID-19 due to their immunosuppressive state and multiple comorbidities. Many present-day studies have reported on the outcomes of COVID-19 positivity in RTR in the developed world (4–10). From developing countries, the data is not sufficient yet (11). To cover this evidence gap, we studied and analyzed clinical manifestations, immunosuppression regimen, treatment, and outcomes in 15 COVID-19 positive RTR in SAMC & PG Institute Indore, India.
Material and Method
This clinical study was conducted in accordance with the principles stated in the Declaration of Helsinki and Declaration of Istanbul. Written informed consent was obtained from all recipients. Confirmed cases: The diagnosis of COVID-19 was confirmed by real-time reverse polymerase chain reaction (RT-PCR) with nasopharyngeal (nasal) and oropharyngeal (throat) swabs (3,12).
Study population: Adult RTR with COVID-19 (age > 18 years) treated from April 1, 2020 to December 15, 2020 were assessed retrospectively.
Clinical severity and assessment parameters
Clinical severity and assessment parameters were divided as follows:
-
Mild: Kidney transplant recipient with uncomplicated upper respiratory tract (URI) infections such as mild symptoms, including cough and fever without shortness of breath or hypoxia.
-
Moderate: Patients demonstrated pneumonia with no signs of disease severity, including fever, cough, dyspnoea, hypoxia with oxygen saturation (SpO2) < 94% (range 90–94%) in room air, and respiratory rate of 24–30/min.
-
Severe: Patients had advanced signs of pneumonia plus one of the following clinical criteria: respiratory rate > 30/min, severe respiratory distress, SpO2 < 90% in room air.
Computerized tomography (CT) severity score (13)
A semi-quantitative CT severity score was calculated for each of the five lobes considering the extent of anatomic involvement as follows: 0, no involvement; 1 < 5% involvement; 2–5 to 25% involvement; 3–26 to 50% involvement; 4–51 to 75% involvement; and 5 to >75% involvement.
-
Mild: Score of less than 25% lobar involvement.
-
Moderate: Score includes involvement of 26–75%.
-
Severe: Score includes patients with more than 75% involvement.
Clinical management protocol: COVID-19.(14)
Detailed clinical history, including comorbidities, was recorded. RTR were followed on daily basis for body temperature changes, vitals, complete blood counts, and additional evaluations as indicated; chest X-ray was obtained daily; target SpO2 was 92–96%.
Anticoagulation: Prophylactic doses of unfractionated heparin or low molecular weight heparin (e.g., enoxaparin, 40 mg per day subcutaneous [SC]) were given.
Hydroxychloroquine (400 mg) 12 hourly was applied on day 1 of admission, followed by 200 mg 12 hourly for 4 days under electrocardiogram (ECG) monitoring; hydroxychloroquine dosage was adjusted based on renal function.
Convalescent plasma (off-label) was given to patients with moderate disease with progressively increasing oxygen requirement despite the use of steroids. The dose of convalescent plasma ranged from 5 to 14 mL/kg (usually a single dose of 200 mL was given as slow infusion over at least 2 h).
Methylprednisolone IV, 0.5 to 1 mg/kg body weight or dexamethasone 0.2–0.4 mg/kg for 3 days was given to all moderate and severe patients (preferably within 48 h of admission if inflammatory markers were increasing or the requirement of oxygen was increasing).
Tocilizumab (off-label): The Interleukin 6 (IL-6) receptor antibody tocilizumab may be given to patients with moderate disease, clinical deterioration, and increased oxygen requirement, or to mechanically ventilated patients not showing improvement despite using steroids. As the long-term safety data of tocilizumab in COVID-19 are unavailable, the following special considerations before its use were included in our study:
-
Presence of increased inflammatory markers (e.g., C-reactive protein [CRP], ferritin, and IL-6).
-
Patients must be monitored carefully post tocilizumab for neutropenia and secondary infections.
-
Tuberculosis and active infections, which must be ruled out before use.
Tocilizumab was applied at 8 mg/kg (maximum 800 mg at one time) diluted in 100-mL Normal Saline (NS), given as slow infusion over 1 h.
Favipiravir: In June 2020, the drug controlling authority of India approved favipiravir for treating mild to moderate COVID-19. A dose of 1800 mg twice a day (bd) on the first day and 800 mg bd for 2 weeks was advised.
Remdesivir: In July 2020, the drug controlling authority of India approved remdesivir for treating mild to moderate COVID-19. A dosage of 200 mg once a day (OD) on the first day and 100 mg OD for next 4 days was suggested.
Discharge policy (15)
In May 2020, the Indian Ministry of Health and Family Welfare (3) issued a revised discharge policy for COVID-19. Criteria for discharge of COVID-19 patients were as follows:
-
A normal chest X-ray and
-
Two consecutive negative test results of COVID-19 RT-PCR.
Home Therapy
We thoroughly selected patients with presenting symptoms, clinical and CT severity scoring on OPD basis. These patients received teleconsultation until resolution of the disease.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences, version 17.0 (SPSS Inc., Chicago, IL). Continuous data are presented as mean ± SD and median and interquartile range (IQR); Student’s t-test was applied to compare two groups.
Results
A total of 15 RTRs tested positive for SARS-CoV-2 during the study period. The median age of RTRs was 42.6 years with male predominance. The recipients presented at a median of 4 years after transplant.
The most common comorbidities included arterial hypertension in 14 patients (94%), diabetes in 5 patients (33%), and both hypertension and diabetes in 3 patients (19%) as depicted in Table 1.
Table 1: Comorbidities in renal transplant recipients with COVID 19.
| S. No. | Comorbidities | Number of patients (N = 15) | Percentage (%) |
|---|---|---|---|
| 1. | Hypertension | 14 | 94 |
| 2. | Diabetes mellitus | 5 | 33 |
| 3. | Hypertension and diabetes mellitus | 3 | 19 |
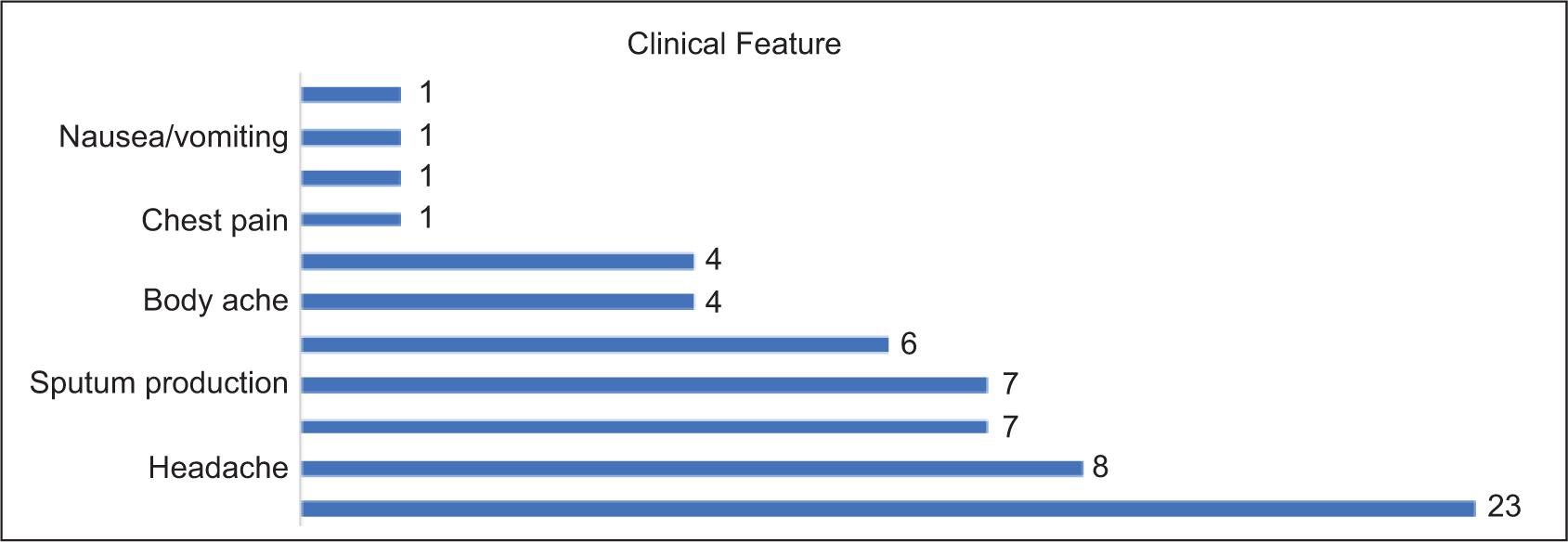
Presenting symptoms (Table 2) included cough (n = 12, 80%), headache (n = 8, 52%), fever and sputum (n = 7, 46%), sore throat (n = 6, 40%), and body ache and breathlessness (n = 4, 26%).
Table 2: Clinical presentation of COVID 19 in renal transplant recipients.
| Clinical features | Number | Percentage (%) |
|---|---|---|
| Cough | 12 | 80 |
| Headache | 8 | 52 |
| Fever | 7 | 46 |
| Sputum production | 7 | 46 |
| Sore throat | 6 | 40 |
| Body ache | 4 | 26 |
| Breathlessness | 4 | 26 |
| Chest pain | 1 | 6 |
| Diarrhea | 1 | 6 |
| Nausea/vomiting | 1 | 6 |
| Loss of taste/smell | 1 | 6 |
Unlike in normal individuals, diarrhea, chest pain, nausea/vomiting, loss of taste, and smell were present in only one patient (6%) as depicted in Figure 1.
Figure 1: Clinical features of COVID-19 in renal transplant recipients.
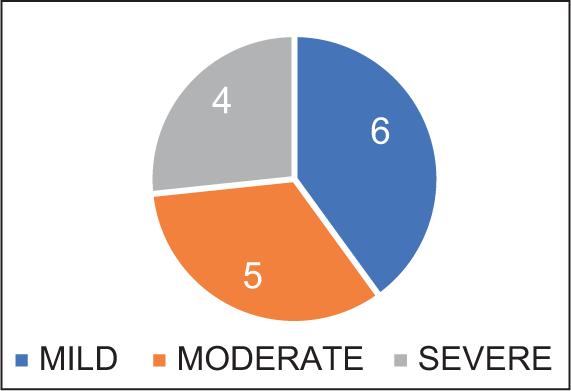
Renal transplant recipients in our study developed mild (n = 6, 40%), moderate (n = 5, 33%), and severe infection (n = 4, 26%) depending on clinical presentation (Figure 2). The disease severity at baseline did not show any significant association with age, baseline laboratory indices, or time from symptoms to RT-PCR report.
Figure 2: Severity score in COVID-19 renal transplant recipients.
Radiological findings
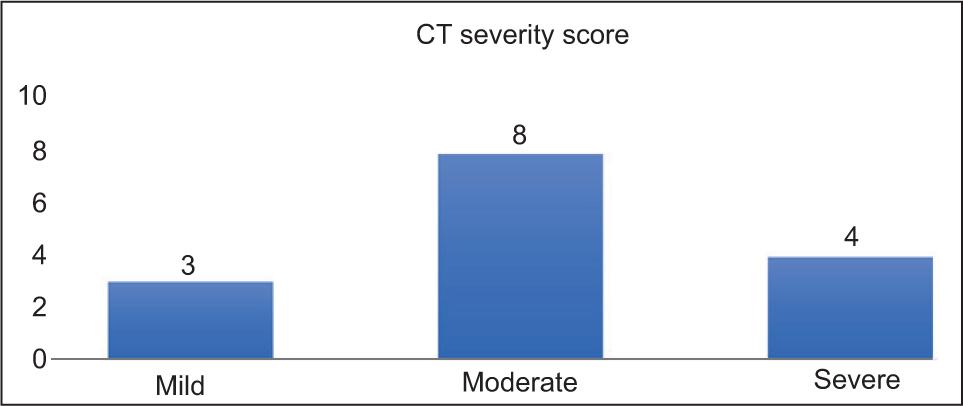
Abnormalities in chest X-ray were seen in 66% (n = 10) patients and was found normal in 33% (n = 5) cases. The commonest CT finding (n = 15) was ground glass opacity. Severity of disease as per CT severity score is depicted in Table 3; most of the patients had moderate CT severity score as shown in Figure 3.
Table 3: CT severity score in COVID-19 renal transplant recipients.
| CT severity score | Number | Percentage (%) |
|---|---|---|
| MILD | 3 | 20 |
| MODERATE | 8 | 53 |
| SEVERE | 4 | 27 |
Figure 3: CT severity score.
Laboratory findings
At presentation, the median hemoglobin was 13 (IQR: 10.1–15.9) gm/dL, total white blood cell count was 4000 (IQR: 2100–10,800) mm, neutrophils 77% (68–86%), lymphocyte 18% (IQR: 12–24%), and platelet count was 126 (IQR: 105–590) × 100/mm3 of blood.
Medical management
Specific treatments with proportion of patients were as follows: azithromycin 100% (n = 15), hydroxychloroquine 67% (n = 10), favipiravir 20% (n = 3), remdesivir 67% (n = 10), tocilizumab 6.7% (n = 1), and convalescent plasma 26.6% (n = 4). Adverse effects such as prolonged corrected QT (QTc) interval requiring early discontinuation of treatment were not observed. Immunosuppressive treatment was modified in the majority of patients. Antimetabolites (mycophenolate/azathioprine) were discontinued in all patients. Calcineurin inhibitors (CNI) were not changed in any patient. Prednisolone dose was increased in 26% (n = 4) patients, while the same dose was continued in the remaining 74% (n = 11) cases. Four patients received convalescent plasma of which two expired and the remaining two were discharged. Standard dose of remdesivir was prescribed to 10 patients, of which one expired and nine were discharged. None of our patients received colchicine, oseltamivir, chloroquine, any traditional medication, antiretroviral drugs (ribavirin, lopinavir/ritonavir, etc.) interferon, or plasmapheresis.
Hospital course and clinical outcome
A total of 26.4% (n=4) cases required admission to intensive care unit (ICU); 8 52% (n = 8) cases needed oxygen supplementation; 6.6% (n = 1) needed noninvasive ventilation; and 13% (n = 2) needed mechanical ventilation, however both patients expired. Acute kidney injury (AKI), defined as increase in creatinine by 0.3 or >50% of baseline value, was seen in 46% (n = 7) patients. AKI was mostly observed in moderate to severe cases and was less common in mild/asymptomatic cases. In all, 6.65% (n = 1) required hemodialysis, which was discontinued after 1 month. In all, 18% (n = 11) patients were discharged from hospital, with a median follow-up done after 28 days. Two (13.2%) patients expired; mortality rate increased to 50% (2/4) for patients in the ICU and 100% (2/2) in case of patients on mechanical ventilation. Mortality was not reported in any COVID-19 RTR treated in OPD. Mortality risk factors included ABO-incompatible transplant, severity of disease, high Coronavirus Disease 2019 (COVID-19) Reporting and Data System (CO-RADS) score on high-resolution computed tomography (HRCT) chest, patients having a history of allograft dysfunction before COVID-19, AKI, and increased inflammatory markers, which included CRP, and ICU/ventilator requirements.
Discussion
COVID-19 has spread rapidly throughout the world, so the global population has been at its risk. It is a well-known fact that RTRs have a higher risk of COVID-19. We presented 15 confirmed RTRs with COVID-19 at our hospital. Although our cohort was small, it was clear that as in the general population, COVID-19 could present in various ways, and the prognosis could vary among RTRs. We had a detailed retrospective study on COVID-19 positive RTRs at our hospital.
It is important to point out that many patients with COVID-19-like symptoms had uneventful OPD treatment for an acute febrile illness like symptoms during the nationwide lockdown, as local laboratory tests could not be performed on regular basis because of resource and testing limitations. Thus, the study conducted at our centre might overestimate mortality rate in Indian RTRs, as possibly many RTRs remained undiagnosed and were never tested or hospitalized.
Although clinical features at presentation were similar to those of the general population, they varied considerably such as fever, cough, sore throat, body ache, and loss of taste and smell sensation. RTRs in our study had high rate of AKI, 56% (n = 8), similar to the reports from the developed world.
It is a well-known fact that T-cell immunity must predominate in controlling viral replication and the disease (16). It is yet not clear whether stopping or modifying all immunosuppressants in transplant recipients is helpful, but based on the above-mentioned theory, we stopped antimetabolite therapy in all patients. Most COVID-19 deaths were associated with acute respiratory distress syndrome (ARDS). Uncontrolled release of cytokines is the likely cause of ARDS. This was evident from the fact that a subgroup of patients with severe COVID-19 may have a cytokine storm syndrome.
Current treatments included supportive care along with hydroxychloroquine, azithromycin, favipiravir, plasma therapy, tocilizumab, and remdesivir (17–19). Mortality in the developed world was associated with the following risk factors: old age (>60 years), lower lymphocyte counts, high IL-6 levels (cut-off value: 65 pg/L), CRP (cut-off value: 100 mg/L), high D-dimer, that is, >960 µg/mL, high procalcitonin test (PCT), higher serum lactate dehydrogenase (LDH) (>300 U/L), thymoglobulin induction therapy, oxygen requirement of ≥6 L/min, mechanical ventilation, elevated serum creatinine before COVID-19, thymoglobulin induction therapy, disease severity at the time of presentation, past treatment for acute rejections, and more than one comorbidity (4–10). Similar risk factors were presented in our study as well. Hemodialysis was required in 6.7% of our patients, which was comparable to 5% patients found in Indian studies as demonstrated by Tatapudi et al. (20).
Most patients developed mild (40%), moderate (33%), and severe disease (37%) in our RTR population, comparable to the recent report of asymptomatic (25%), mild (28%), moderate (34%), and severe (12%) COVID-19 in solid organ transplant (SOT) recipients (21). Our study demonstrated that carefully selected RTR with mild COVID-19 could be managed at home with good outcomes as described in an Italian and UK cohort (5,22,23). This finding supports home treatment that could be imparted to RTRs having mild COVID-19; this could be relevant for developing worlds having limited healthcare resources.
In India, the mortality rate in hospitalized COVID-19 non-transplant patients appeared to be significantly lower than transplant patients (24–26). Differences were less pronounced in patients having severe disease. Mortality rate of 4.8–33% has been reported in SOT recipients with COVID-19 as described in various studies from the developed world (4–10).
However, in our study, RTR population appeared to have a lower mortality (13.38%), compared to the reports of transplant recipients with COVID-19 from Italy with an overall mortality rate of 25% among admitted patients (17). This was similar to the mortality of 14.6% from an Indian study conducted by Jha et al. (27). Mortality was 100% in our patients who were put on mechanical ventilatory support, similar to the results demonstrated by Jasuja et al. in India (28). Larger studies are required to fully understand the mortality risk in transplant recipients with COVID-19.
Higher mortality in RTR with COVID-19 could be due to the use of immunosuppressants by such patients and having higher comorbidities (94% vs. 70%) (3). Comparison of outcomes of COVID-19 in dialysis population to COVID-19 in transplant patients is of additional relevance. Published data from various Indian dialysis centers have reported the mortality rate ranging from 12% to 37.8% (29,30).
Our study had certain limitations. Foremost being that there was no uniform protocol for the treatment of COVID-19 positive patients. Treatment regimens continued to evolve based on new evidence and more data published in due course because of mounting COVID-19 in RTRs. In summary, our data provided relevant information regarding outcomes in RTRs with COVID-19 in developing countries such as India. Thus, this may serve to assess the risks and improve outcomes in case of COVID-19 positive RTRs on global level.
Conclusions
Mortality rate in COVID-19 positive RTRs appears to be more than patients who were not immunocompromised. Higher mortality was observed among those having ABO-incompatible transplants, having a previous history of rejection, and patients requiring intensive care with mechanical ventilatory support. Early cessation of antimetabolites (mycophenolate mofetil [MMF] and azathioprine), early diagnosis and treatment with antiviral drugs (favipiravir and remdesivir) in viral replicative phase, and stepping up the dose of steroid therapy could help in recovery from COVID-19 in RTRs.
Conflict of Interest
The authors declare no conflicts of interest with respect to this study.
REFERENCES
1. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. New Eng J Med. 2020 Feb;382(8);727–33. 10.1056/NEJMoa2001017
2. Kute V, Ramesh V, Shroff S, Guleria S, Prakash J. Deceased-donor organ transplantation in India: Current status, challenges, and solutions. Exp Clin Transplant. 2020 Jul 1;18(Suppl 2):31–42. 10.6002/ect.rlgnsymp2020.L6
3. Ministry of Health and Family Welfare. Available from: https://www.mohfw.gov.in/. Accessed September 13, 2020.
4. Cravedi P, Mothi SS, Azzi Y, Haverly M, Farouk SS, Pérez-Sáez MJ, et al. COVID-19 and kidney transplantation: Results from the TANGO International Transplant Consortium. Am J Transplant. 2020 Nov;20(11):3140–8. 10.1111/ajt.16185
5. Bossini N, Alberici F, Delbarba E, Valerio F, Manenti C, Possenti S, et al. Kidney transplant patients with SARS-CoV-2 infection: The Brescia Renal COVID Task Force experience. Am J Transplant. 2020 Nov;20(11):3019–29. 10.1111/ajt.16176
6. Avery RK. COVID-19 therapeutics for solid organ transplant recipients; 6 months into the pandemic: Where are we now? Transplantation. 2021;105(1):56–60. 10.1097/TP.0000000000003519
7. Akalin E, Azzi Y, Bartash R, Seethamraju H, Parides M, Hemmige V, et al. Covid-19 and kidney transplantation. New Eng J Med. 2020 Jun 18;382(25):2475–7. 10.1056/NEJMc2011117
8. Caillard S, Anglicheau D, Matignon M. An initial report from the French SOT COVID Registry suggests high mortality due to Covid-19 in recipients of kidney transplants. Kidney Int. (Published online ahead of print August 24, 2020) 2020 Dec 98(6):1549–58. 10.1016/j.kint.2020.08.005
9. Stephanie GY, Rogers AW, Saharia A, Aoun M, Faour R, Abdelrahim M, et al. Early experience with COVID-19 and solid organ transplantation at a US high-volume transplant center. Transplantation. 2020 Nov;104(11):2208. 10.1097/TP.0000000000003339
10. Hilbrands LB, Duivenvoorden R, Vart P, Franssen CF, Hemmelder MH, Jager KJ, et al. COVID-19-related mortality in kidney transplant and dialysis patients: Results of the ERACODA collaboration. Neph Dialysis Transplant. 2020 Nov;35(11):1973–83.
11. Shingare A, Bahadur MM, Raina S. COVID-19 in recent kidney transplant recipients. Am J Transplant. 2020 Nov;20(11):3206–9. 10.1111/ajt.16120
12. Kates OS, Fisher CE, Stankiewicz-Karita HC, Shepherd AK, Church EC, Kapnadak SG, et al. Earliest cases of coronavirus disease 2019 (COVID-19) identified in solid organ transplant recipients in the United States. Am J Transplant. 2020 Jul;20(7):1885–90. 10.1111/ajt.15944
13. National Clinical Management Protocol COVID-19. Clinical management protocol: COVID-19 [Internet]. Available from: https://www.mohfw.gov.in/pdf/ClinicalManagementProtocolforCOVID19.pdf. Accessed 15 December, 2020.
14. Francone M, Iafrate F, Masci GM, Coco S, Cilia F, Manganaro L, et al. Chest CT score in COVID-19 patients: Correlation with disease severity and short-term prognosis. Eur Radiol. 2020 Dec;30(12):6808–17. 10.1007/s00330-020-07033-y
15. Revised discharge policy for Covid-19 [Internet]. Available from: https://www.mohfw.gov.in/pdf/ReviseddischargePolicyforCOVID19.pdf. Accessed December 15, 2020.
16. Uematsu J, Sakai-Sugino K, Kihira-Nakanishi S, Yamamoto H, Hirai K, Kawano M, et al. Inhibitions of human parainfluenza virus type 2 replication by ribavirin and mycophenolate mofetil are restored by guanosine and S-(4-nitrobenzyl)-6-thioinosine. Drug Discov Therap. 2019 Dec 31;13(6):314–21. 10.5582/ddt.2019.01084
17. Alberici F, Delbarba E, Manenti C, Econimo L, Valerio F, Pola A, et al. Management of patients on dialysis and with kidney transplant during COVID-19 coronavirus infection. Kidneys. 2020;9(2):117–20. 10.22141/2307-1257.9.2.2020.203411
18. Devaux CA, Rolain JM, Colson P, Raoult D. New insights on the antiviral effects of chloroquine against coronavirus: What to expect for COVID-19? Int J Antimicrob Agents. 2020 May 1;55(5):105938. 10.1016/j.ijantimicag.2020.105938
19. Patel A, Shah K, Dharsandiya M, Patel K, Patel T, Patel M, et al. Safety and efficacy of tocilizumab in the treatment of severe acute respiratory syndrome Coronavirus-2 pneumonia: A retrospective cohort study. Indian J Med Microbiol. 2020 Jul 1;38(1):116–22. 10.4103/ijmm.IJMM_20_298
20. Tatapudi RR, Kopparti VR, Poosapati A, Metta S, Gongada AR, Vedulla B. SARS-CoV-2 Infection in kidney transplant recipients: A single-centre study of 20 cases from India. Int J Nephrol. 2021 Nov 5;2021: Article ID 2243095. 10.1155/2021/2243095
21. Ali T, Al-Ali A, Fajji L, Hammad E, Nazmi A, Alahmadi I, et al. Coronavirus disease-19: Disease severity and outcomes of solid organ transplant recipients: Different spectrums of disease in different populations. Transplantation. 2021 Jan 1;105(1):121–7. 10.1097/TP.0000000000003433
22. Husain SA, Dube G, Morris H, Fernandez H, Chang JH, Paget K, et al. Early outcomes of outpatient management of kidney transplant recipients with coronavirus disease 2019. Clin J Am Soc Nephrol. 2020 Aug 7;15(8):1174–8. 10.2215/CJN.05170420
23. Felldin M, Søfteland JM, Magnusson J, Ekberg J, Karason K, Schult A, et al. Initial report from a Swedish high-volume transplant center after the first wave of the COVID-19 pandemic. Transplantation. 2021 Jan 1;105(1):108–14. 10.1097/TP.0000000000003436
24. Mohan A, Tiwari P, Bhatnagar S, Patel A, Maurya A, Dar L, et al. Clinico-demographic profile & hospital outcomes of COVID-19 patients admitted at a tertiary care centre in north India. Indian J Med Res. 2020 Jan 1;152(1):61. 10.4103/ijmr.IJMR_1788_20
25. Chatterjee P. Is India missing COVID-19 deaths? Lancet. 2020 Sep 5;396(10252):657. 10.1016/S0140-6736(20)31857-2
26. Jha PK, Yadav DK, Siddini V, Bansal SB, Sharma R, Anandh U, et al. A retrospective multi-center experience of renal transplants from India during COVID-19 pandemic. Clin Transplant. 2021 Jul;35:e14423. 10.1111/ctr.14423
27. Jasuja S, Sagar G, Bahl A, Verma S. COVID-19 infection clinical profile, management, outcome, and antibody response in kidney transplant recipients: A single centre experience. Int J Nephrol. 2021 Oct 3;2021: Article ID 3129411, 10 pages. 10.1155/2021/3129411
28. Mishra V, Burma AD, Das SK, Parivallal MB, Amudhan S, Rao GN. COVID-19-hospitalized patients in Karnataka: Survival and stay characteristics. Indian J Public Health. 2020 Jun 1;64(6):221. 10.4103/ijph.IJPH_486_20
29. Deshpande R, Dash S, Bahadur MM, Thamba A, Pathan AK, Dave K, et al. Study of COVID-19 pandemic in representative dialysis population across Mumbai, India: An observational multicentric analysis. J Ass Physicians India. 2020 Oct 1;68(10):13–7.
30. Trivedi M, Shingada A, Shah M, Khanna U, Karnik ND, Ramachandran R. Impact of COVID-19 on maintenance haemodialysis patients: The Indian scenario. Nephrology. 2020 Dec;25(12):929–32. 10.1111/nep.13760