
Download
ORIGINAL ARTICLE
Clinicopathologic Spectrum of Xanthogranulomatous Pyelonephritis: A Single Center Experience over 8 Years
Farhat Abbas1, Summyia Farooq1, Gul Aalmeen1, Muzamil Latief2*, Mohsin Wani1
1Pathology Division, Government Medical College, Srinagar, Kashmir, India;
2Nephrology Division, Government Medical College, Srinagar, Kashmir, India
Abstract
Xanthogranulomatous pyelonephritis (XGP) is a chronic pyelonephritis subtype in which destruction of the renal parenchymal occurs, resulting in progressive loss of kidney functions. Although middle age is the predominant age group affected, but it can be spotted at any age. There is accumulation of macrophages (lipid-laden), leading to renal parenchymal destruction and fibrosis. In this study, we present our data of 15 patients who had undergone nephrectomy and had biopsy-proven XGP. XGP constituted 4.53% of the 331 nephrectomies performed for infective causes over a period of 8 years. All our patients had undergone unilateral total nephrectomy. Demographic and clinical data were analyzed after taking consent from all the patients. The age range of patients in our study was 18–65 years with a mean age of 43.93 ± 13.86 years. Ten (66.6%) of our patients were females. Diabetes was present in 40% of the patients. Three patients had imaging, suggestive of pyonephrosis, 3 had perinephric collection and 9 patients (60%) had concomitant nephrolithiasis. All the kidneys were grossly enlarged and were nonfunctional on renal scintigraphy. XGP is a form of chronic pyelonephritis, which, although less common, is devastating because of destruction of the renal parenchyma and associated morbidity. Clinicoradiologic correlation cannot be overemphasized. Definitive diagnosis is established through histopathologic examination.
Key words: pyelonephritis, pyonephrosis, XGP
Received: 9 October 2021; Accepted after Revision: 8 November 2021; Published: 7 April 2022
Author for correspondence: Muzamil Latief, Nephrology Division, Government Medical College, Srinagar, Kashmir, India. Email: muzamillatief.b@gmail.com
How to cite: Abbas F, et al. Clinicopathologic Spectrum of Xanthogranulomatous Pyelonephritis: A Single Center Experience over 8 Years. J Ren Hepat Disord. 2022 6(1):32–35.
Doi: http://dx.doi.org/10.15586/jrenhep.v6i1.135
Copyright: Abbas F, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
The clinical spectrum of Xanthogranulomatous pyelonephritis (XGP) is varied similar to its etiology. XGP was first described by Schlagenhaufer more than a century ago (1). Owing to its varied presentation, the differential diagnosis is also wide. It is a chronic pyelonephritis subtype in which destruction occurs to the renal parenchyma, resulting in progressive loss of kidney functions. Although middle age is the predominant age group affected, but it can be spotted at any age. XGP is usually unilateral; however, bilateral conditions have also been reported (2–4). The primary reason for XGP is obstructive pathology, which most commonly is nephrolithiasis. In children it can be secondary to congenital abnormalities of the kidney and urinary tract (5,6). The condition is usually seen in females and people having chronic comorbidity, such as diabetes and autoimmune diseases, or are on immunosuppressants (7–9). There is accumulation of macrophages (lipid-laden), leading to renal parenchymal destruction and fibrosis. The process of inflammation and damage could extend beyond the kidney and may involve surrounding structures. The kidney is usually nonfunctional, and surgical intervention in the form of nephrectomy is the only definitive treatment (10). In this study, we present our data of 15 patients who had undergone nephrectomy and had biopsy-proven XGP.
Materials and Methods
We present 15 patients of XGP, diagnosed on the basis of histopathologic findings. These patients constituted 4.53% of the 331 nephrectomies performed for infective causes over a period of 8 years at our center. All our patients had undergone unilateral total nephrectomy. All the patients consented for this study. Demographic and clinical records were analyzed after having consent from all the 15 patients. Specimens were fixed in 10% formalin and grossed. Paraffin-embedded sections were cut into 5-μm slices, followed by hematoxylin and eosin (H&E) staining. Sections were studied under light microscope in both low and high magnification.
Results
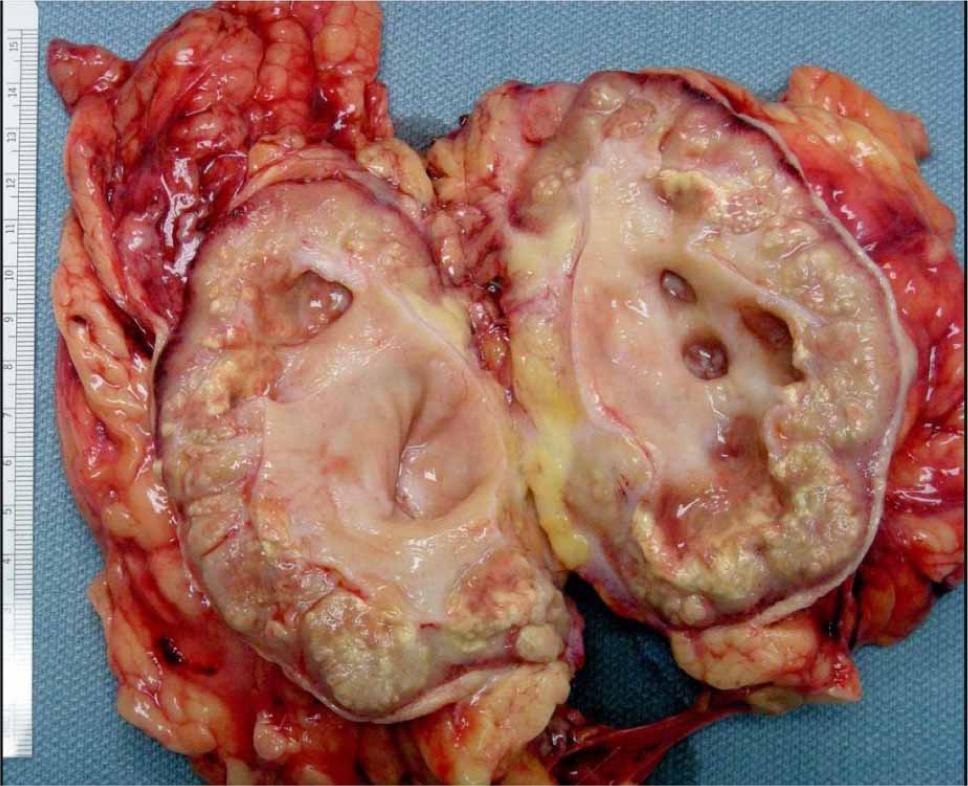
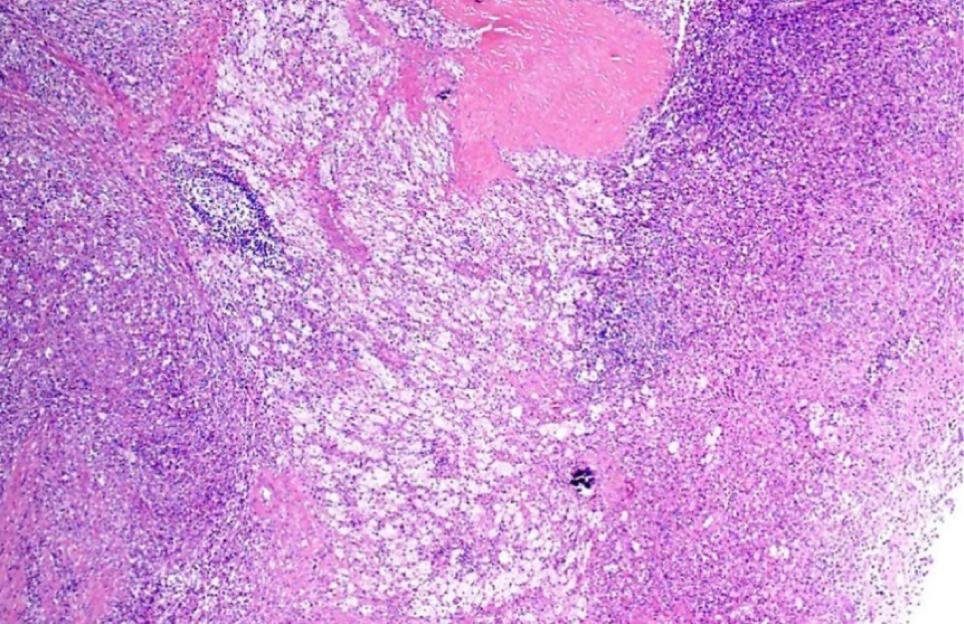
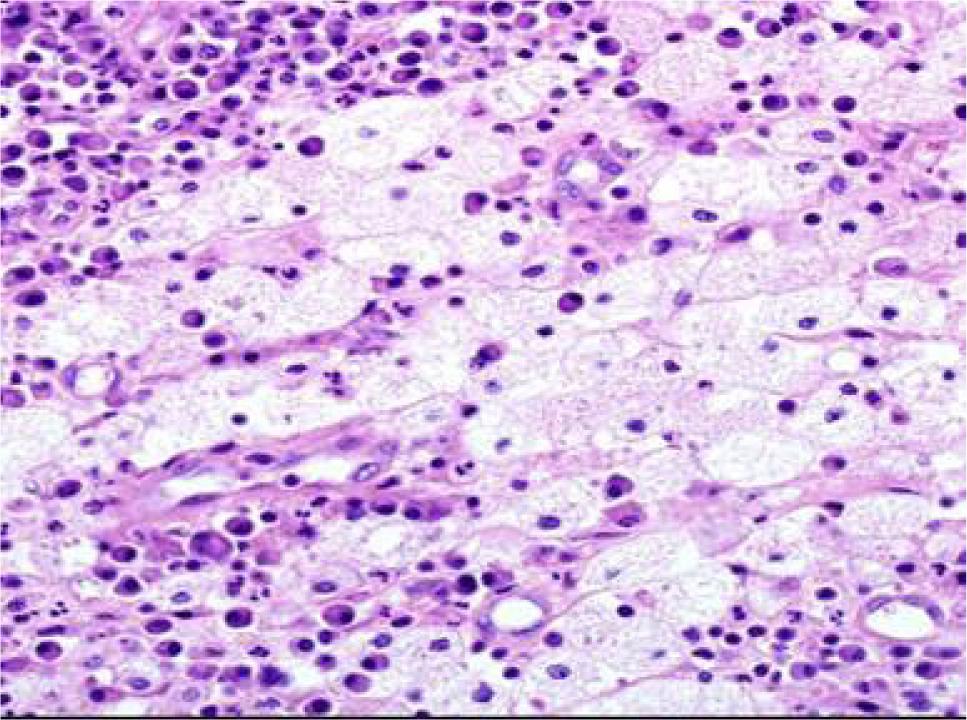
The age range in our study was 18–65 years with a mean age of 43.93 ± 13.86 years. All patients underwent open procedure. Ten (66.6%) of our patients were females. Diabetes was present in 40% of the patients. Tables 1 and 2 show the clinical and biochemical parameters of the patients. None of our patients had bilateral disease. Flank pain in all cases and fever in 11 patients (73.3%) were the commonest symptoms reported at presentation. All the patients had undergone ultrasound examination, followed by contrast-enhanced computed tomography (CECT) and radioscintigraphy (diethylene triamine penta-acetic acid [DTPA] aerosol). Urine culture reports were positive in nine patients. Three patients had imaging suggestive of pyonephrosis, three had perinephric collection, and nine (60%) had concomitant nephrolithiasis. All the kidneys were grossly enlarged. None of our patients had a neoplastic lesion on biopsy. Figure 1 shows gross specimen of XGP kidney. Figures 2 and 3 show light microscopic findings on low and high power magnification, respectively.
Table 1: Clinical parameters of patients.
| Parameter | N |
|---|---|
| Age (Mean ± SD) | 43.93 ± 13.86 |
| Male, n (%) | 5 (33.3%) |
| Female, n (%) | 10 (66.6%) |
| Diabetes, n (%) | 6 (40%) |
| Hypertension, n (%) | 9 (60%) |
| Hematuria, n (%) | 5 (33.3%) |
| Fever, n (%) | 11 (73.3%) |
| Flank pain, n (%) | 15 (100%) |
| Abdominal lump, n (%) | 4 (26%) |
| Nephrolithiasis, n (%) | 9 (60%) |
Table 2: Biochemical parameters of patients.
| Parameters | Mean ± SD |
|---|---|
| Hemoglobin (g/dL) | 10.66 ± 1.33 |
| Creatinine (mg/dL) | 1.5 ± 0.39 |
| White blood cells (WBC) | 14,600 ± 4990/µL |
| Platelets | 2.36 ± 0.93/µL |
| Albumin | 3.81 ± 0.68 g/dL |
| Urine culture | Positive: 9 patients |
| Negative: 6 patients | |
| Pyuria | 15 patients |
Figure 1: Gross photograph showing nephrectomy specimen with poor corticomedullary differentiation, dialated renal pelvicalyceal system with deposition of yellowish specks limited to the renal parenchyma and sparing perinephric fat in XGP patient.
Figure 2: Photomicrograph image showing the renal parenchyma infiltrated with dense inflammation and foam cells on low magnification, suggestive of XGP on H&E staining.
Figure 3: Photomicrograph image showing foam (xanthoma) cells and lymphoplasmacytic inflammation on H&E staining in XGP patient on high magnification.
Discussion
XGP is a relatively rare subtype of chronic pyelonephritis with varying occurrences, which range between 0.6% and 1% as reported in literature (1). XGP is usually diffused (involving most of the kidney), and focal variant is less common. All age groups may be affected, but it is more commonly spotted in middle-age and elderly patients. XGP has been more commonly reported in females (11). Our study too observed that XGP is more common in females as compared to males. All the patients had unilateral presentation, as bilateral presentation is rarely encountered (2). Obstruction of the urinary tract and recurrent urinary tract infection (UTI) are common in XGP (1). A study conducted in India reported that nephrolithiasis was observed in 90% of XGP patients (12). Similarly, in our study nephrolithiasis was observed in nine (60%) patients. Diabetes mellitus, urinary stasis because of obstructive pathologies, renal neoplastic lesions, and immunocompromised attributes predispose patients to XGP (13,14). In the present study, diabetes was diagnosed in six (40%) patients and none of our patients was on immunosuppressive medications or had underlying malignancy. Varying clinical presentations have been observed in different studies. All the patients had abdominal pain on presentation, which is similar to most of the published series (7,12,14). In a recent study, pyonephrosis and perinephric abscess were observed in 25.0% and 7.5% patients, respectively (12), whereas in our study, three (20%) patients had pyonephrosis and three had perinephric collection. In a study conducted in Turkey, leukocytosis was observed in one (7.7%) patient, pyuria was diagnosed in six (46.1) patients, and 46.1% patients were anemic (15). Korkes et al. (5) analyzed 41 patients of XGP, in which anemia, pyuria, and leukocytosis were reported in 63%, 57.6%, and 41% of cases, respectively. In our study 11 (73.3%) patients were anemic, leucocystosis was diagnosed in 9 (60%), and all the patients had pyuria. In a study conducted by Kundu et al. (12), XGP was diffused in 31 (77.5%) patients and focal in 9 (22.5%) cases whereas in our study, diffused XGP was observed in 11 (73.3%) patients, which was similar to their study. Moreover, they observed biopsy diagnosis of XGP in 23 (57.5%) patients, 10 (25.0%) patients had pyonephrosis with XGP, 3 (7.5%) had XGP with diabetic nodular glomerulosclerosis, and 1 patient had renal cell carcinoma with concomitant XGP(12). In our study, pyonephrosis with XGP was noted in three patients whereas another three had perinephric collection. Diabetic glomerulosclerosis with XGP was observed in one of the six diabetic patients in our study, and none of our patients had neoplastic lesions. XGP has been divided into three stages: stage I is nephric XGP, which is confined to the renal parenchyma; stage II is perinephric XGP, having involvement of the anterior perirenal fascia, or Gerota’s fascia; and stage III is paranephric XGP, having involvement of the pararenal space and retroperitoneal structures (16). In the present study, 12 patients had stage I disease and 3 patients had stage II disease. Histopathologic examination of XGP determined an admixture of lipid-laden foamy macrophages with infiltration of varying mixtures of inflammatory cells along with fibrotic changes and cholesterol deposition. We too observed most of these changes in our specimens.
Conclusion
XGP is a form of chronic pyelonephritis, which, although less common, is devastating, because it causes destruction to the renal parenchyma and associated morbidity. Clinicoradiologic correlation, pertaining to both clinical and radiologic findings, cannot be overemphasized, and definitive diagnosis is established through histopathology.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to research, authorship and/or publication of this article.
Funding
No funding was received for this study. All the patients consented for this study.
REFERENCES
1. Siddappa S, Ramprasad K, Muddegowda MK. Xanthogranulomatous pyelonephritis: A retrospective review of 16 cases. Korean J Urol. 2011;52:421–4. 10.4111/kju.2011.52.6.421
2. Tsai KH, Lai MY, Shen SH, Yang AH, Su NW, Ng YY. Bilateral xanthogranulomatous pyelonephritis. J Chin Med Assoc. 2008 Jun;71(6):310–4. 10.1016/S1726-4901(08)70128-X.
3. Das DP, Pal DK. Co-existing malakoplakia and xanthogranulomatous pyelonephritis of kidney: Two different spectrum of same disease process. Urol Ann. 2016;8:252–4. 10.4103/0974-7796.179242.
4. Bansal K, Sureka B, Jain V, Arora A. Bilateral xanthogranulomatous pyelonephritis: Morphologically rotund, functionally lame! Indian J Nephrol. 2015 Jul–Aug;25(4):255–6. 10.4103/0971-4065.149960.
5. Korkes F, Favoretto RL, Bróglio M, Silva CA, Castro MG, Perez MD. Xanthogranulomatous pyelonephritis: Clinical experience with 41 cases. Urology. 2008 Feb;71(2):178–80. 10.1016/j.urology.2007.09.026
6. Nicola R, Menias CO. Urinary obstruction, stone disease, and infection. In: Hodler J, Kubik-Huch RA, von Schulthess GK, editors. Diseases of the abdomen and pelvis 2018–2021: diagnostic imaging. Cham, Switzerland: Springer; 2018. pp. 223–228.
7. Li L, Parwani AV. Xanthogranulomatous pyelonephritis. Arch Pathol Lab Med. 2011;135:671–4. 10.5858/2009-0769-RSR.1
8. Grainger RG, Longstaff AJ, Parsons MA. Xanthogranulomatous pyelonephritis: A reappraisal. Lancet. 1982;1(8286):1398–1401. 10.1016/S0140-6736(82)92511-9
9. Levy M, Baumal R, Eddy AA. Xanthogranulomatous pyelonephritis in children. Etiology, pathogenesis, clinical and radiologic features, and management. Clin Pediatr. 1994;33(6):360–6. 10.1177/000992289403300609
10. Addison B, Zargar H, Lilic N, Merrilees D, Rice M. Analysis of 35 cases of xanthogranulomatous pyelonephritis. ANZ J Surg. 2015;85:150–3. 10.1111/ans.12581
11. Al-Ghazo MA, Ghalayini IF, Matalka II, Al-Kaisi NS, Khader YS. Xanthogranulomatous pyelonephritis: Analysis of 18 cases. Asian J Surg. 2006;29:257–61. 10.1016/S1015-9584(09)60099-3
12. Kundu R, Baliyan A, Dhingra H, Bhalla V, Punia RS. Clinicopathological spectrum of xanthogranulomatous pyelonephritis. Indian J Nephrol. 2019 Mar–Apr;29(2):111–5. 10.4103/ijn.IJN_50_18
13. Tüysüz G, Tayfun F, Canpolat F, Zeytun H, Goya C, Keles¸ AN, et al. A case of xanthogranulomatous pyelonephritis mimicking Wilms tumor. Turk J Pediatr. 2015;57:409–12. PubMed: 27186708
14. Leoni FA, Kinleiner P, Revol M, Zaya A, Odicio A. Xanthogranulomatous pyelonephritis: Review of 10 cases. Arch Esp Urol. 2009;62:259–71. 10.4321/s0004-06142009000400001
15. Çaliskan S, Özsoy E, Kaba S, Koca O, Öztürk MI. Xanthogranulomatous pyelonephritis. Arch Iran Med. 2016 Oct;19(10):712–4. PMid: 27743436.
16. Malek RS, Elder JS. Xanthogranulomatous pyelonephritis: A critical analysis of 26 cases and of the literature. J Urol. 1978 May;119(5):589–93. 10.1016/s0022-5347(17)57559-x.