
Download
Original Article Nephrology
Epidemiological, Clinical, Therapeutic, and Evolutionary Aspects of Acute Kidney Damage during Severe Malaria in Children at the Borgou Departmental Teaching Hospital (Benin)
Séraphin Ahoui1*, Alphonse Noudamadjo2, Gerard Kpanidja2, Evariste Eteka1, K.O. Auguste Akoto1, Falilatou Agbeille2, Muriel Toutche1, Aristide Dah3, Julien Didier Adedemy2, Joseph Agossou2
1Department of Nephrology, Faculty of Medicine, University of Parakou, Parakou, Benin;
2Department of Pediatrics, Faculty of Medicine, University of Parakou, Parakou, Benin;
3Parakou Medico-Social Training School, Parakou, Benin
Abstract
Malaria is an endemic pathology with several complications, including kidney damage. The objective of this work was to study kidney damage during severe malaria in children at the pediatrics department of the Borgou Departmental Teaching Hospital (Borgou DTH), Benin in 2021. This was a longitudinal study carried out over 4 months from June 1, 2021 to September 30, 2021 (with 1 month of recruitment from June 1 to July 1, 2021) at the pediatric department of the Borgou DTH. The study included children aged 1 month–15 years, hospitalized for Plasmodium falciparum malaria with at least one clinical manifestation of malaria severity established by the World Health Organization in 2000 and whose parents had given their informed consent. The damage was established by urinary sedimentation using urine dipstick and urinary cap and serum creatinine. Acute kidney injury (AKI) was intended and classified according to the Kidney Disease Improving Global Outcomes (KDIGO) criteria. The dependent variable was the presence of at least one clinical, biological, and functional impairment. Follow-up was regular for up to 3 months. Lost to follow-up were excluded. Predictors of occurrence were identified. Statistical difference was considered significant at P < 0.05. Of the 164 children hospitalized for severe malaria during the study period, 72 had at least one renal impairment, with a frequency of 43.90%. The average age of the children was 44.93 months. On urine dipstick, 76.39% of the patients had hemoglobinuria and 55.56% had albuminuria. Urinary cap revealed 44% granular cylindruria and 32% crystalluria. AKI was detected in 4.54% patients. Recovery was complete in all follow-up cases. The predictors of kidney damage were coma ( P = 0.017), jaundice ( P = 0.007), thrombocytopenia ( P = 0.021), and long hospital stay ( P = 0.008). Kidney damage in severe malaria is frequent. Early diagnosis and prompt treatment are fundamentals of rapid and complete recovery of kidney functions.
Key words: children, kidney disease, malaria, predictors, Parakou
Received: 9 November 2021; Accepted after Revision: 3 March 2022; Published: 26 April 2022
Author for correspondence: Séraphin Ahoui, Faculty of Medicine, University of Parakou, CDE Rd., Parakou, Benin. Email: drserahoui@gmail.com
How to cite: Ahoui S, et al. Epidemiological, Clinical, Therapeutic, and Evolutionary Aspects of Acute Kidney Damage during Severe Malaria in Children at the Borgou Departmental Teaching Hospital (Benin). J Ren Hepat Disord. 2022 6(1):48–55.
Doi: http://dx.doi.org/10.15586/jrenhep.v6i1.137
Copyright: Ahoui S, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
Malaria is an erythrocytopathy caused by hematozoa Plasmodium, transmitted by the bite of Anopheles mosquito. It is an endemic infection that has spread globally, affects millions of people living in the tropics, and constitutes a major public health problem (1). In Africa, it is a leading cause of death in children aged less than 5 years. In 2019, the World Health Organization (WHO) estimated 229 million malaria cases globally with a total number of 405,000 deaths, of which 67% (approximately 274,000) were child deaths aged less than 5 years (1). In Benin, according to the Fifth Demographic and Health Survey of 2017–2018 (DHSB-V), the prevalence of malaria in children aged 6–59 months was 39% with an overall prevalence of 45% in the pediatric department of Borgou Departmental Teaching Hospital (Borgou DTH) (2).
Plasmodium falciparum is the species implicated in the severe forms of malaria as well as child deaths because of malaria (3). It causes visceral complications, particularly in the brain, liver, and kidneys (4). Kidney damage because of severe malaria is varied. These are usually fluid and electrolyte disturbances, glomerular involvement such as glomerulonephritis, and abnormalities in renal function such as acute kidney injury (AKI) (5,6).
Acute kidney injury is the most frequently described functional manifestation (3), the incidence of which in the pediatric population is variable (depending on the factors such as the definition of AKI and the cohort studied), arriving at 46%. In Benin, few studies have been conducted on kidney injury in severe malaria. The only study carried out on AKI associated with severe malaria (AKI-M) was in Cotonou, Benin, stating a prevalence of 0.56% (7). The present work was undertaken in 2021 to intensify knowledge and broaden horizons on renal damage in malaria. The objective was to study renal damage during severe malaria in children at the pediatric department of Borgou DTH in Benin.
Patients and Study Methods
Study Method
This was a longitudinal study with a prospective data collection carried out for 4 months from June 1, 2021 to September 30, 2021 (with a recruitment month of June 1–July 1, 2021) at the pediatric department of Borgou DTH. The study focused on patients hospitalized in the pediatric department of the Borgou DTH for Plasmodium falciparum malaria with at least one clinical manifestation of severity of malaria established by the WHO in 2000. Children aged 1 month to 15 years, with severe Plasmodium falciparum malaria, and for whom one of the parents or a legal representative had given informed consent, were included in the study. Children aged less than 1 month or more than 15 years or with uncomplicated malaria were excluded from the study. Children who dropped out of follow-up were also excluded from the study. An exhaustive recruitment was carried out of patients who meet the inclusion criteria.
As diagnostic criteria, severe Plasmodium falciparum malaria was identified by a positive rapid diagnostic test (RDT) and/or a thick drop and blood smear positive for Plasmodium falciparum associated with severity criteria, including the presence of manifestations of severity as established by the WHO (8). The dependent variable was the presence of acute anatomical and/or functional renal damage. Independent sociodemographic, clinical, paraclinical, diagnostic, and therapeutic variables were also studied
Renal involvement, according to the Kidney Disease Improving Global Outcomes (KDIGO) criteria, entailed the presence of an anatomoclinic and/or functional feature such as:
-
renal-type edema,
-
diuretic abnormalities with a urine volume of <0.5 mL/kg/h for 6 h,
-
albuminuria/hemoglobinuria/hematuria/leukocyturia with dipstick test/urinary sedimentation, and
-
AKI according to the KDIGO 2012 criteria; either an elevated creatinine level of at least 3 mg/L in 48 h or more than 1.5 times the baseline value in 1 week and/or diuresis of less than 0.5 mL/kg/h for 6–12 h (9).
Collection method and technique
The data were collected using a survey questionnaire that was completed at the time of patient’s admission to the pediatric ward. The questionnaire was administered through a structured face-to-face interview with admitted child’s one of the parents (mother preferable). Sociodemographic data were collected through a face-to-face interview with parents. Clinical data was taken from interview and physical examination. Blood and urine samples were collected in case of all patients. A urine dipstick test was performed for all children with severe malaria on admission (Day 0 [D0]) and D2, and for follow-up on D7 or before discharge from hospital on D30 and D90 for those who had presented with at least one anomaly. In case of an anomaly, urine sediment was performed prior to urine dipstick test. Tests for uremia and serum creatinine were performed on admission (D0) and D2 for all children admitted with severe malaria, and on D7 and before discharge from hospital on D30 and D90 for the follow-up of those who had presented with AKI.
Diuresis was monitored daily. Urine collection was done using “urinocols” or sterile jars, depending on the age and functional ability of patients. The collection team comprised three general practitioners, a pediatrician, and a nephrologist.
Data processing and analysis
After data collection, double entry was made in the software “Épi Data 3.1fr”. The collected data were exported into Microsoft Excel 2016 for analysis. The analysis was also done with STATA SE, version 15.0. Qualitative variables were expressed as percentage. Quantitative variables if normally distributed were expressed as an average with standard deviation, otherwise they were expressed as median and its interquartile range.
A comparative analysis of the variables considered as risk predictors was carried out. Pearson’s chi-square and Fischer’s exact test were performed for each qualitative variable. A variable was retained for the construction of multivariate model by conditional logistic regression when the degree of significance (P-value) was less than 0.20.
Collinearity was tested between explanatory variables retained after univariate analysis in order to eliminate those correlated to each other. In case of correlation, we kept only one of these correlated variables for the rest of modeling, choosing the one with the most significant P-value.
A conditional logistic regression model was performed to explain predictors of risk for kidney injury. Explanatory variables selected after collinearity research were integrated into a stepwise descending multivariate model.
The threshold of statistical significance was set at 0.05. At each step, a likelihood ratio test was performed. The ranking of explanatory variables was based on odds ratio (OR) and their 95% confidence interval (95% CI).
Ethical considerations
The research protocol was approved by the local ethics committee for biomedical research of the University of Parakou (LECBR-UP). Agreement of competent authorities at various levels, in this case director of Borgou DTH and chief physician of the pediatric service, was obtained before data collection in the service. Oral or written consent of a parent was obtained before administration of the questionnaire. In addition, anonymity and confidentiality of the information collected was assured.
Results
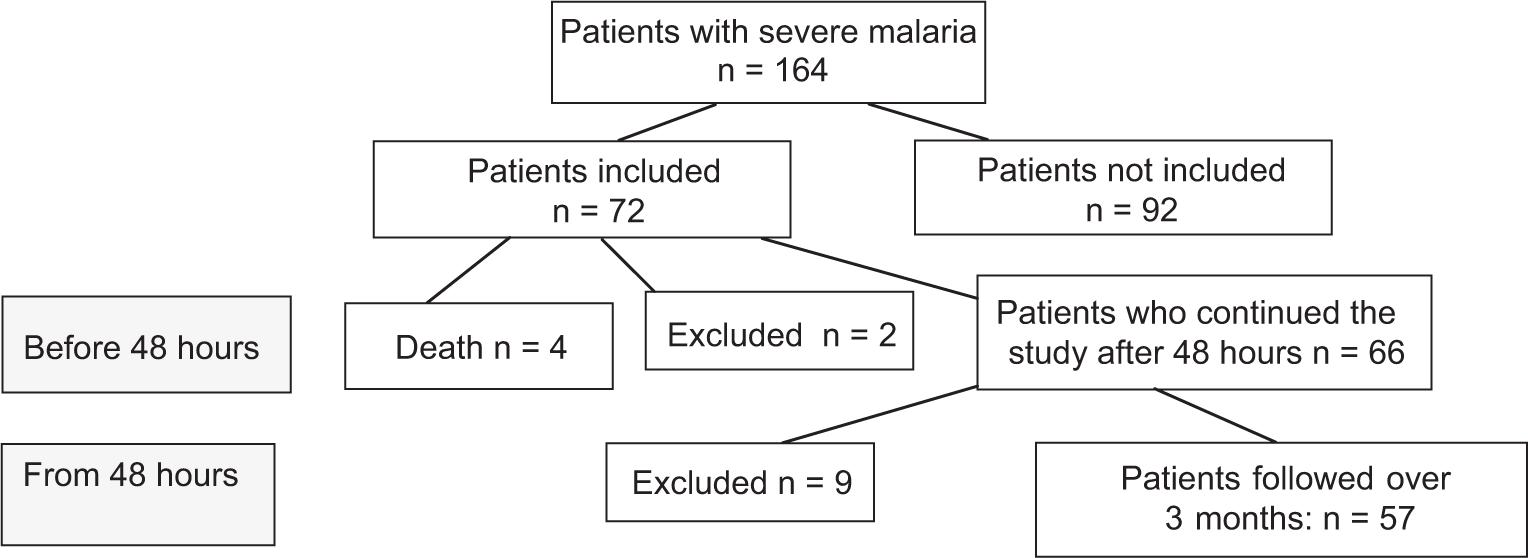
During the study period, 164 children hospitalized for severe malaria were included in our study (Figure 1).
Figure 1: Flow diagram of patients with severe malaria at the Borgou Departmental Teaching Hospital included in the study in 2021.
General characteristics of the study population
The average age of children was 36 months ± 32.57 months (range: 3 months to 13 years). Of these 164 children, 88 (53.6%) were boys, with a sex ratio of 1:15.
Frequency of acute kidney injury
Overall incidence of acute kidney damage
During our study period, 72 children (43.90%), out of 164 children hospitalized for severe malaria, had kidney damage.
Relative frequency of breaches
Renal impairment from urine sediment
Renal impairment noted from urine dipstick test at admission was hemoglobinuria (76.39%), albuminuria (55.56%), leukocyturia (6.94%), and hematuria (4.17%).
Of the 72 children, 40 (55.56%) presented with albuminuria, of which 29 (40.27%) and 11 (15.27%) had ++ and +++ severity level, respectively.
Of the 72 children, 50 developed hemoglobinuria, with a severity of + (12.50%), ++ (15.27%), and +++ (48.61%).
Urinary density of 1.015 and 1.020 were, respectively, found in 12 (16.67%) and 20 (27.78%) of the admitted children.
Urine was diluted with a specific gravity of 1005 and 1010 in 10 (13.89%) and 21 (29.16%) children, respectively.
Urine was concentrated with a specific gravity of 1025 and 1030 in 5 (6.94%) and 4 (5.56%) children, respectively.
Average pH of urine was 6.14 with extremes of 5 and 8.
Urinary pH was acidic (<5.8) in 15 (20.83%), normal (5.8–6.5) in 45 (62.50%), and basic (6.5–8) in 12 (16.67%) children.
Urinary sediment was abnormal in 50 (69.44%) patients. Renal lesions found on urinary sediment were granular cylindruria (44.44%), crystalluria (32.00%), bacteriuria (22%), white blood cells (18.06%) and red blood cells (9, 72%).
Functional impairment
Upon admission, impaired renal function was found in five (6.94%) patients. The average serum creatinine at admission was 5.40 ± 5.26 mg/L with extremes of 1.30–38.58 mg/L. One case of death was recorded of these five patients.
Of the remaining 66 children, a persistence increase in serum creatinine of more than 3 mg/L was noted from the second day of hospitalization in three children with impaired renal function on admission. According to the KDIGO criteria, frequency of AKI on D2 was 4.54%. Stages 2 and 3 of AKI were noted in one and two children, respectively. Relating to abnormalities in urine output upon admission, two of the 72 children had presented abnormalities in urine output such as anuria and oliguria (one case each), and both of these kids had AKI. Table 1 shows the distribution of cases of renal damage according to clinical elements of urinary sediment, and functional plan.
Table 1: Distribution of children with severe malaria with kidney damage according to clinical elements, urine sediment, and functional plan at Borgou DTH in 2021 (n = 72).
| Number | Percentage | |
|---|---|---|
| Diuresis abnormalities | 02 | 2.77 |
| Anuria | 01 | 1.39 |
| Oliguria | 01 | 1.39 |
| Urine sediment | ||
| Urine dipstick | ||
| Hemoglobinuria | 50 | 76.39 |
| + | 09 | 12.50 |
| ++ | 11 | 15.27 |
| +++ | 35 | 48.61 |
| Albuminuria | 40 | 55.56 |
| ++ | 29 | 40.27 |
| +++ | 11 | 15.27 |
| Leukocyturia | 05 | 6.94 |
| Hematuria | 03 | 4.17 |
| Urine density | ||
| Low (1.005 and 1.010) | 31 | 43.06 |
| Normal (1.015 and 1.020) | 32 | 44.44 |
| Concentrated (1.025 and 1.030) | 09 | 12.50 |
| pH | ||
| Acidic (<5.8) | 15 | 20.83 |
| Normal (5.8–6.5) | 45 | 62.50 |
| Basic (6.5–8) | 12 | 16.67 |
| Urine count | ||
| Red blood cells | 07 | 9.72 |
| White blood cells | 13 | 18.06 |
| Bacteria | 16 | 22.22 |
| Granular cylinders | 32 | 44.44 |
| Crystals | 23 | 32.00 |
| Alteration in renal function | ||
| On admission (n = 72) | 05 | 6.94 |
| 48 h later (D2) (n = 66) | 03 | 4.54 |
Characteristics of children with renal damage during severe malaria
Sociodemographic characteristics of patients
The average age of children with renal impairment because of severe malaria was 44.93 months (range: 3 months–13 years).
Among 72 children with renal impairment because of severe malaria, 37 (51.39%) were boys with a sex ratio of 1:6.
Clinical features of children with renal damage
The most common reason for consultation on admission was pallor, reported in 33.33% cases (n = 24). Seizures, asthenia, and lethargy were reported in 20.83% (n = 15), 18.06% (n = 13), and 9.72% (n = 7) cases, respectively.
Of the 72 patients, 42 (58.33%) were hospitalized between 3 and 7 days of the onset of symptoms—33.33% patients (n = 24) before 3 days and 8.33% (n = 6) after 7 days. Comorbidities were found in 27 children (37.5%), including bronchopneumonia in 15 children (20.83%), urinary tract infection (UTI) in 6.94% (n=5), salmonellosis in 5.56% (n=4), and meningitis and gastritis in 1 child (1.39%) each. Table 2 shows distribution according to reason for consultation, time of admission, and comorbidities.
Table 2: Distribution of children with severe malaria and kidney damage according to reason for consultation, admission time, and comorbidities at the Borgou DTH in 2021 (n = 72).
| Number | Percentage | |
|---|---|---|
| Reason for consultation | ||
| Pallor | 24 | 33.33 |
| Convulsions | 15 | 20.83 |
| Asthenia | 13 | 18.06 |
| Lethargy | 7 | 9.72 |
| Altered consciousness | 5 | 6.94 |
| Urine dirty broth | 4 | 5.56 |
| Jaundice | 1 | 1.39 |
| Agitation | 1 | 1.39 |
| Time to admission | ||
| <3 days | 24 | 33.33 |
| 3–7 days | 42 | 58.33 |
| ≥7 days | 6 | 8.33 |
| Comorbidities | ||
| Bronchopneumonia | 5 | 6.94 |
| Malnutrition | 9 | 12.50 |
| Urinary tract infection | 3 | 4.16 |
| Digestive infection/sepsis | 4 | 5.56 |
| Salmonellosis | 4 | 5.56 |
| Meningitis | 1 | 1.39 |
| Gastritis | 1 | 1.39 |
On physical examination, the general condition was altered in all children. Of the 72 patients, 68.06% had a febrile state, and the average temperature was 38.2ºC ± 0.97ºC (range 36.1–40.8ºC). Among these children, tachycardia and polypnea were found in 94.44% and 81.94% cases, respectively. Blood pressure was normal in all children.
Palpal pallor was present in 95.83% cases (n = 69) and palpebral pallor was found in 88.89% (n=64) cases. Renal-like edema was present in 4.17% cases.
Diuresis was preserved in 70 cases (97.22%) and 12.5% (n=9) had poor nutritional status. Splenomegaly and hepatomegaly were observed in 33 (45.83%) and 18 (25.00%) cases, respectively.
Considering clinical manifestations of seriousness according to the WHO criteria, following observations were recorded: 80.56% cases of respiratory distress, 37.50% cases of jaundice, 33.33% cases of coma, and 27.78% cases of repeated convulsions. Gross hemoglobinuria was observed in 19.44%, lethargy in 12.50%, abnormal bleeding in 2.78%, and cardiovascular collapse in 2.78% cases.
Table 3 shows distribution according to the results of physical examination and clinical manifestations of severity according to the WHO.
Table 3: Distribution of children with severe malaria and kidney damage according to the results of the physical examination and clinical manifestations of severity according to WHO at the Borgou DTH in 2021 (n = 72).
| Number | Percentage | |
|---|---|---|
| Physical signs | ||
| Palmar pallor | 69 | 95.83 |
| Tachycardia | 68 | 94.44 |
| Palpebral pallor | 64 | 88.89 |
| Polypnea | 59 | 81.94 |
| Febrile state | 49 | 68.06 |
| Splenomegaly | 33 | 45.83 |
| Hepatomegaly | 18 | 25.00 |
| Poor nutritional status | 9 | 12.50 |
| Edema | 3 | 4.17 |
| Diuresis abnormalities | 2 | 2.78 |
| Clinical manifestations of severity (WHO) | ||
| Respiratory distress | 58 | 80.56 |
| Icterus | 27 | 37.50 |
| Coma | 24 | 33.33 |
| Repeated seizures | 20 | 27.78 |
| Gross hemoglobinuria | 14 | 19.44 |
| Lethargy | 9 | 12.50 |
| Cardiovascular collapse | 2 | 2.78 |
| Abnormal bleeding | 2 | 2.78 |
Paraclinical characteristics of children with renal impairment
The average parasite density was 10,609 parasites/µL ± 229,695.34 parasites/µL, with extremes of 320–1,734,311 parasites/µL. Plasmoduim falciparum was the only species found in the blood smear. Severe anemia was present in 83.33% of cases. The mean hemoglobin level was 5.40 g/dL ± 6.02 g/dL, with extremes of 2.80–9.40 g/dL. Thrombocytopenia was present in 95.84% of children. Manifestations of paraclinical severity, according to the WHO, were as follows: hypoglycemia in 11.11% cases, hyperparasitaemia in 9.72% cases, and AKI was found in 6.94% cases. Table 4 shows distribution according to paraclinical manifestations.
Table 4: Distribution of children with severe malaria and renal impairment according to paraclinical manifestations at Borgou DTH in 2021 (n = 72).
| Number | Percentage | |
|---|---|---|
| Paraclinical manifestations | ||
| Thrombocytopenia | 69 | 95.84 |
| Severe anemia | 60 | 83.33 |
| Hyponatremia | 2 | 2.78 |
| Paraclinical manifestations of severity (WHO) | ||
| Hypoglycemia | 8 | 11.11 |
| Hyperparasitemia | 7 | 9.72 |
| Acute renal injury | 5 | 6.94 |
Therapeutic characteristics
Prior to admission, proportion of children had received antipyretic (66.67%), antianemic (19.44%), antibiotic (19.44%), and herbal (15.28%) medicines. Children had also received combinations of artemisinin (15.28%), quinine salts (12.50%), and vitamin complexes (9.72%).
Of the 72 patients 13 (18.06%) had not received any treatment before admission. Upon admission, the hygiene and dietary measures instituted were salt and sodium restriction in 3 (4.16%) patients and hyperhydration in 57 (79.16%) patients.
During hospitalization, the management of severe malaria was based on injection artesunate to all patients and therapeutic combinations based on artemisinin to 94.44% of patients.
Antibiotics and anticonvulsants were administered to 45.83% and 33.33% of patients, respectively. Paracetamol (an antipyretic) was prescribed to 18.06%, red blood cell transfusion to 83.33%, iron to 91.67%, nutritional intake to 16.67%, and multivitamins to 2.78% of patients. Furosemide at a dosage of 2 mg/kg/day was administered to 5.55% and sodium bicarbonate was prescribed to 4.16% of patients.
Evolutionary characteristics
The length of hospitalization of children ranged from 1 day to 19 days with an average of 3.92 days. Of the 72 patients, stay of less than 3 days was in the case of 33.33% patients, ranging between 3 and 7 days in 54.16% of patients, and that of more than 7 days was in 12.50% patients.
In children who presented with renal impairment because of severe malaria, a favorable outcome was recorded in 57 (79.17%) patients, 4 cases (5.56%) of death were recorded, and 11 patients (15.27%) lost of view. Compared to the evolution of renal damage, a favorable development was noted. The urine output was normal for all the 66 children followed before their discharge from the hospital.
Urine dipstick test was performed on D2 in 66 children and 6 cases of hemoglobinuria and 2 cases of albuminuria were recorded.
Before discharge from hospital and at various follow-up appointments, no pathological element was detected with urine dipstick test.
Of the five children who had impaired renal function on admission, three had a consistently high serum creatinine on D2. One case of death was recorded among these five patients and improvement was observed in rest of the cases on D2.
Serum creatinine level achieved on D30 in three children was normal and the same was noted on D90. Progression to chronic kidney disease was not noted in any patient.
Identification of risk predictors for the onset of kidney damage in severe malaria
In univariate analysis, the occurrence of renal damage in severe malaria in children was statistically associated with the presence of jaundice (1.35–5.98; P = 0.004), thrombocytopenia (1.20–10.09; P = 0.021), and length of hospital stay (1.16–4.54; P = 0.009)
In multivariate analysis, the occurrence of renal damage during severe malaria in children was statistically associated with the presence of icterus (1.34–6.77; P = 0.007), thrombocytopenia (1.23–14.39; P = 0.021), coma (0.19–0.84; P = 0.017), and hospital stay of more than 3 days (1.07–1.62; P = 0.008). The data are presented in Table 5.
Table 5: Predictors of the occurrence of renal impairment in severe malaria in children at Borgou DTH in 2021 after univariate and multivariate analyses.
| Univariate analysis | Multivariate analysis | |||||
|---|---|---|---|---|---|---|
| PR | 95% CI | P | ORajusté | 95% CI | P | |
| Jaundice | 0.004 | 0.007 | ||||
| Non | 1 | 1 | ||||
| Oui | 2.85 | 1.35–5.98 | 3.02 | 1.34–6.77 | ||
| Thrombocytopenia | 0.021 | 0.021 | ||||
| No | 1 | |||||
| Yes | 3.48 | 1.20–10.09 | 4.21 | 1.23–14.39 | ||
| Coma | ||||||
| No | 1 | |||||
| Yes | 0.59 | 0.31–1.13 | 0.110 | 0.40 | 0.19–0.84 | 0.017 |
| Length of hospitalization (in days) | ||||||
| <3 | 1 | - | 1 | |||
| 3–7 | 2.30 | 1.16–4.54 | 0.009 | 1.32 | 1.07–1.62 | 0.008 |
| 7–10 | 3.82 | 1.10–13.21 | ||||
| >10 | - | - | ||||
OR: odds ratio; 95% CI: 95% confidence interval; PR: Prevalence Ratio.
Discussion
Commentary and comparison of the results obtained
Frequency
We identified 72 children with kidney damage in severe malaria from a total number of 164 patients hospitalized for severe malaria according to the WHO criteria. This corresponds to an overall frequency of 43.90%. This overall frequency is similar to that of 41.80% determined by Kéita et al. (10) in 2014 in Senegal. It is lower than that of 59% determined by Oshomah-Bello et al. (11) in Nigeria in 2017. It is higher than that of 32.4% defined by Afolayan et al. (12) in Nigeria in 2017 , and 17.4% of Esezobor et al. (13) in Nigeria in 2012. This could be explained by the short size of our sample and the short duration of present study. In addition, anomalies were identified at several levels (clinical–biological and functional levels).
As for AKI 48 h after admission, the frequency was 4.54%. This frequency was close to 6.6% established by Moussa Tondi et al. (14) in Niger in 2016. . The frequency of AKI in the present study remained higher than that of 2% demonstrated by Ephraim et al. (15) in Ghana in 2018, 0.7% by Essola et al. (16) in Gabon in 2017, and 0.56% by Lalya et al. (7) in Benin in 2012. AKI was selected according to the KDIGO criteria and not only because of increase in serum creatinine. Some patients had already presented with impaired renal function. Variation in our frequency could also be due to small sample size of the present study.
The length of hospital stay ranged from one to 19 days with an average stay of 3.92 days. Essola et al. and Lalya et al. reported an average hospital stay of 10.8 days and 13 days, respectively (7,18), which is much higher compared to our results. Renal damage was less, and recovery progressed favorably with good management of severe malaria.
In this study, complete recovery of renal function was noted in patients with AKI and no case of chronic kidney disease was observed. These results were consistent with those reported by Lalya et al. in Benin (7). In contrast, Shah et al. (17) observed only 64% complete recovery of renal function with chronicity of 5%. The same was true in the study conducted by Moussa Tondi et al. (14) in Niger, which reported 74% recovery of renal function and 4% progression to chronicity. Early management and search for damage on several levels facilitated rapid recovery and regression of lesions.
Predictors of onset of renal impairment
Risk factors of renal impairment in severe malaria found in this study were jaundice ( P = 0.007), coma ( P = 0.017), thrombocytopenia ( P = 0.021), and the length of hospital stay ( P = 0.008). In India, Zaki et al. (18) found the following risk factors similar to those of this study: coma (P = 0.0072), jaundice ( P = 0.021), and hyperbilirubinemia (P = 0.0046).. Jaundice in severe malaria releases free bilirubin into the blood and blocks kidney tubules, leading to tubular necrosis. Coma is the result of blocking of microcirculation in the brain. This phenomenon can also take place at the kidney level, which justifies that in the event of cerebral damage there can be renal damage (19). Concerning hospital stay, the more it increases, the more the patient is subjected to numerous therapies, which can lead to kidney damage and is linked to complication of malaria (20).
This was the first study conducted at Borgou DTH (Benin) on the subject of renal damage in malaria, and constituted basis for the future research. However, it has some limitations such as short duration and systematic failure to perform ultrasound to detect morphological abnormalities.
Conclusion
Renal damage in malaria is common and varied in children. In fact, in this study, hemoglobinuria was the most common condition. It constituted a serious complication of infection and must be pursued systematically, especially in children aged less than 5 years, the main subjects of this study. If the diagnosis is made early and treatment is implemented quickly, the progression is toward rapid and complete recovery of kidney function.
Conflict of interest
None. No funding was received for this study.
Authors’ contribution
All the authors contributed equally to this study.
REFERENCES
1. World Health Organization (WHO). World malaria report 2020: 20 Years of global progress and challenges. Geneva, Switzerland: WHO; 2020.
2. Enquêtes Démographiques et de Santé. Résultats d’un atelier de l’utilisation des données des Enquêtes Démographiques et de Santé [Internet]. [cited 2020 Nov 14]. Rockville, MD: ICF; Sep 2020. Available from: www.Dhsprogram.com.
3. Trampuz A, Jereb M, Muzlovic I, Prabhu RM. Clinical review: Severe malaria. Crit Care. 2003;7(4):315–23. 10.1186/cc2183
4. Elsheikha HM, Sheashaa HA. Epidemiology, pathophysiology, management and outcome of renal dysfunction associated with plasmodia infection. Parasitol Res. 2007;101(5):1183–90. 10.1007/s00436-007-0650-4
5. Eiam-Ong S, Sitprija V. Falciparum malaria and the kidney: A model of inflammation. Am J Kidney Dis. 1998;32(3):361–75. 10.1053/ajkd.1998.v32.pm9740151
6. Kamath N, Iyengar A. Infections and the kidney: A tale from the tropics. Pediatr Nephrol. 2018;33(8):1317–26. 10.1007/s00467-017-3785-2
7. Lalya F, Sagbo G, Bagnan L, Alihonou F, Tohodjede Y, Almeida M, et al. L’insuffisance rénale aiguë associée au paludisme chez l’enfant au Centre National Hospitalier Universitaire Hubert Koutoucou Maga de Cotonou, Benin. Rev Afr Anesth Med Urgence. 2014;19(1):39–42.
8. Gachot B, Bruneel F, Berth C. Paludisme grave. Revue du Praticien. 2001;51(6):638–43. 10.1016/s0246-0289(09)50990-5
9. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Inter Suppl. 2012;2(1):1–138. 10.1038/kisup.2012.1
10. Kéita Y, Cissé M, Sylla A, Ly F, Boiro D, Ndongo A, et al. La néphropathie liée au paludisme grave à plasmodium falciparum chez l’ enfant dans deux services pédiatriques universitaires sénégalais : à propos de 79 cas. J Afr Pediatr Genet Med. 2017;3:38-43.
11. Oshomah-bello E, Paed F, Esezobor C, Paed F, Solarin A, Paed F, et al. Acute kidney injury in children with severe malaria is common and associated with adverse hospital outcomes. J Trop Pediat. 2019:66(2):1–8. 10.1093/tropej/fmz057
12. Afolayan F, Adedoyin O, Abdulkadir M, Ibrahim O, Biliaminu S, Mokuolu O, et al. Acute kidney injuries in children with severe malaria a comparative study of diagnostic criteria based on serum cystatin C and creatinine levels. Sultan Qaboos Univ Med J (SQUMJ). 2020;20(4):e312–7. 10.18295/squmj.2020.20.04.006
13. Esezobor C, Ladapo T, Osinaike B, Ebun F, Lesi A. Paediatric acute kidney injury in a tertiary hospital in Nigeria : Prevalence, causes and mortality rate. Plos One. 2012;7(12):1–6. 10.1371/journal.pone.0051229
14. Moussa Tondi Z, Moussa H, Garba M, Abdou I, Salamatou N, Soumeila I, et al. Insuffisance rénale aiguë au cours du paludisme grave de l’enfant : expérience des services de pédiatrie des hôpitaux de la ville de Niamey (Niger). Néphrologie Thérapeutique. 2017;13(5):361–2. 10.1016/j.nephro.2017.08.221
15. Ephraim R, Adoba P, Sakyi S, Aporeigah J, Fondjo L, Botchway F, et al. Acute kidney injury in pediatric patients with malaria: A prospective cross-sectional study in the Shai-Osudoku District of Ghana. Saudi J Kidney Dis Transplant. 2020;31(1):235–44. 10.4103/1319-2442.279946
16. Essola L, Mowangue PS, Minko J, Soami V, Sima ZA, Ngomas JF. Prise en Charge de l’insuffisance rénale aiguë dans le Paludisme Grave de l’Enfant au centre Hospitalier Universitaire de Libreville. Une Étude de 12 Cas. Health Sci Dis. 2019;20(4):57–61. Retrieved from https://www.hsd-fmsb.org/index.php/hsd/article/view/1475
17. Shah P, Vanikar A, Kasat P, Gumber M, Trivedi H, Rasiklal Doshi G, et al. Malaria induced acute renal failure: A single center experience. Saudi J Kidney Dis Transplant. 2010;21(6):1088–91. PMid: 21060178.
18. Zaki S, Shenoy P, Shanbag P, Mauskar A, Patil A, Nagotkar L. Acute renal failure associated with malaria in children. Saudi J Kidney Dis Transpl. 2013;24(2):303–8. 10.4103/1319-2442.109585
19. Van Slambrouck C, Salem F, Meehan S, Chang A. Bile cast nephropathy is a common pathologic finding for kidney injury associated with severe liver dysfunction. Kidney Int. 2013;84(1):192–97. https://pubmed.ncbi.nlm.nih.gov/23486516/
20. World Health Organization (WHO). Severe malaria. Trop Med Int Health. 2014;19:7–131. 10.1111/tmi.12313_2