
Download
ORIGINAL ARTICLE: NEPHROLOGY
Paraquat-associated Severe Acute Kidney Injury—Study from India
Manjusha Yadla*, K. Manu, K.V. Anupama, B. Rajasekhar
Department of Nephrology, Gandhi Medical College, Hyderabad, Telangana, India
Abstract
To analyze the outcomes of severe acute kidney injury in patients with paraquat ingestion. This retrospective analysis of case records was done in our institute, a tertiary care government teaching hospital, over a period of 4 years. Of the total 1310 acute paraquat poisonings during this period, severe acute kidney injury (AKI), referred for nephrology management was observed in 60 patients. Common symptoms at presentation include vomiting, oral ulcers, and abdominal pain. Oliguric AKI was present in 26%. Need for renal replacement therapy was observed in 95% of the cases. Mortality was observed in 38 of the 60 patients (68%). Factors associated with mortality on Cox regression analysis include amount of consumption. Estimated duration of survival on analysis curves was 8 days in 50% after admission and 15 days after consumption in 50%. Paraquat poisoning is associated with grave outcomes of morbidity and mortality. Severity of AKI is significant in this poisoning. Amount of consumption, latency of referral play a major role in outcomes.
Key words: severe acute kidney injury, paraquat ingestion, poisoning, renal replacement therapy
Received: 20 December 2021; Accepted after Revision: 2 November 2022; Published: 13 December 2022
Author for correspondence: Manjusha Yadla, Department of Nephrology, Gandhi Medical College, Hyderabad, Telangana, India. Email: manjuyadla@gmail.com
How to cite: Yadla M, et al. Paraquat-associated Severe Acute Kidney Injury—Study from India. J Ren Hepat Disord. 2022 6(2):14–23
DOI: 10.15586/jrenhep.v6i2.140
Copyright: Yadla M, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Background
Paraquat is a herbicide commonly used in agriculture practice in the Indian subcontinent. Paraquat use in India was approved for nine crops, but because of the ease and effectiveness of its use, it is currently being used for 25 crops grown. Paraquat is a powerful desiccant, and chemically its falls in the group of bipyridilium herbicides, which are also called “quaternary ammonium salts” or “quats.” The WHO, PAN, IRIS, US EPA, and ToxNet have recognized paraquat as a dangerous herbicide. Despite global efforts, it is being widely used in agricultural and nonagricultural practices in India. Almost all Indian states have reported dangerous outcomes due to paraquat poisoning, and states such as Kerala have banned paraquat along with endosulfan.
Paraquat poisoning can have a myriad of manifestations including airway and respiratory complications to acute kidney injury (AKI).
Aim
To determine the outcomes of patients presenting with severe acute kidney injury due to paraquat poisoning.
Patients and Methods
Design
It is a retrospective study of case records of all patients admitted with paraquat poisoning and Nephrology referral.
Setting
This study was done at a tertiary care Government Teaching hospital over a period of 4 years. All those patients with AKI who were referred to Nephrology services were included in the study.
Demographic data, amount of paraquat consumption, nature of poisoning, clinical features, severity of renal insufficiency, and the need for renal replacement therapy (RRT) were analyzed.
Results
Of the total 1310 paraquat poisoning cases admitted to our center over a period of 4 years, 60 patients were referred to the nephrology department for management of severe renal failure. Nature of poisoning was suicidal in majority (86%), and very few were accidental or homicidal in nature. Paraquat is an easily available and commonly used pesticide, the side effects of which are known to agricultural community and hence an easily available suicidal chemical. Mean age of the group was 27 years. The majority were men, 42:18. The time duration of referral from local hospital to our center varied between 24 h and >6 days; the initial management was given at local hospital. Most common symptoms at presentation involved the presence of oral ulcers in the gastrointestinal system, vomiting, and pain in the abdomen. Among renal symptoms, oliguria was the most common, and anuria was infrequent. Hypotension was infrequent at admission, and during hospitalization, majority of the patients developed multiorgan involvement with liver dysfunction and respiratory failure. Of the 60 patients, 57 needed kidney replacement therapy. The baseline characteristics and statistics are presented in Table 1 and Table 2.
Table 1: Baseline characteristics for hospital admission.
| Characteristics | Number (n = 60) |
|---|---|
| Sex | |
| Male | 42 |
| Female | 18 |
| Mode of poisoning | |
| Accidental | 7 |
| Homicide | 1 |
| Suicidal | 52 |
| Presenting symptoms | |
| Breathlessness | 4 |
| Abdominal pain | 13 |
| Oliguria | 16 |
| Vomiting | 25 |
| Icterus | 3 |
| Oral ulcer | 23 |
| Melena | 2 |
| Anuria | 1 |
| Dysphagia | 8 |
| Altered sensorium | 2 |
| SOB | 2 |
| Renal symptoms | |
| Anuria | 1 |
| Nonoliguria | 10 |
| Nonoliguric AKI | 14 |
| Oliguria | 35 |
| Urine albumin | |
| Nil | 38 |
| Trace | 20 |
| Present (+/++) | 2 |
| Type of RRT | |
| HD | 52 |
| HD and PD | 2 |
| PD | 3 |
| No RRT | 3 |
| Other organ involvement | |
| Liver/Lungs (one organ) | 24 |
| Liver + Lungs (two organ) | 13 |
| Ventilator support | 25 |
| Cause of death | |
| MODS | 19 |
| Respiratory failure | 17 |
| Sudden cardiac death | 1 |
| Recovery | |
| Complete | 20 |
| Partial | 3 |
| Outcome | |
| Death | 38 |
| Recovered | 22 |
AKI, acute kidney injury; HD, hemodialysis; MODS, multiple organ dysfunction syndrome; PD, peritoneal dialysis; RRT, renal replacement therapy; SOB, shortness of breath.
Table 2: Statistical results for patients.
| Characteristics | Mean |
|---|---|
| Age | 27.32 ± 9.94 |
| Consumption amount | 73.17 ± 34.47 |
| Systolic BP (mm in Hg) | 120.73 ± 10.63 |
| Diastolic BP (mm in Hg) | 77.33 ± 7.78 |
| Latent time to referral (days) | 6.33 ± 1.7 |
| Day stay | 7.77 ± 5.23 |
| Total day | 14.11 ± 5.41 |
| Serum creatinine at admission (mg/dL) | 6.37 ± 2.49 |
| Hemoglobin (g/dL) | 11.51 ± 1.56 |
| Total leukocyte count | 10,978.33 ± 3524.21 |
| Serum potassium (meQ/L) | 4.14 ± 0.51 |
| PH | 7.34 ± 0.07 |
| Serum bicarbonate (meQ/L) | 14.12 ± 4.26 |
| pCO2 | 25.10 ± 5.32 |
| pO2 | 95.10 ± 15.32 |
| Total bilirubin | 3.39 ± 3.14 |
| Direct bilirubin | 2.14 ± 2.09 |
| SGOT | 78.20 ± 59.29 |
| SGPT | 87.53 ± 68.08 |
| Alkaline phosphatase | 141.38 ± 119.07 |
| Anion gap | 15.48 ± 5.72 |
| Urine output | 683.33 ± 515 |
| Duration of RRT | 3.76 ± 2.18 |
RRT, renal replacement therapy; SGOT, glutamic-oxaloacetic transaminase; SGPT, serum glutamate pyruvate transaminase.
Mortality in our group was 63% (38/60). On univariate analysis, nature of poisoning, amount consumed, and latency period of referral time showed a significant association with mortality. Mortality was observed in those with suicidal nature and who consumed larger amounts, >100 mL (which predominantly was mixed with soft drinks or locally made toddy), and delayed presentation or referral to a tertiary care center. Other parameters that showed a significant association with mortality were elevated WBC, hypoxemia, liver dysfunction, multiorgan involvement, and persisting oliguria. On further analysis using Cox regression multivariate analysis, the factors found significant were amount of consumption, presence of vomiting, and liver dysfunction. Other factors such as hypoxemia, need for ventilation, and lab parameters were not found to be associated with mortality on multivariate analysis. Factors associated with mortality are listed in Table 3.
Table 3: Factors associated with mortality.
| Characteristics | Death (n = 38) | Recovery (n = 22) | P |
|---|---|---|---|
| Age | 25.13 ± 6.70 | 31.09 ± 13.23 | 0.059 |
| Sex | |||
| Male | 28 (73.7%) | 14 (63.6%) | 0.560 |
| Female | 10 (26.3%) | 8 (36.4%) | |
| Mode of poisoning | |||
| Accidental | 2 (5.3%) | 5 (22.7%) | 0.046* |
| Homicide | 0 (0.0%) | 1 (4.5%) | |
| Suicidal | 36 (94.7%) | 16 (72.7%) | |
| Consumption amount | 93.16 ± 26.52 | 38.63 ± 11.25 | 0.0001* |
| Presenting symptoms | |||
| Breathlessness | 2 (9.1%) | 2 (5.3%) | 0.619 |
| Abdominal pain | 6 (15.8%) | 7 (31.8%) | 0.197 |
| Oliguria | 10 (26.3%) | 6 (27.3%) | 1.000 |
| Vomiting | 18 (47.4%) | 7 (31.8%) | 0.286 |
| Icterus | 3 (7.9%) | 0 (0.0%) | 0.292 |
| Oral ulcer | 14 (36.8%) | 9 (40.9%) | 0.788 |
| Melena | 1 (2.6%) | 1 (4.5%) | 1.000 |
| Anuria | 1 (2.6%) | 0 (0.0%) | 1.000 |
| Dysphagia | 5 (13.2%) | 3 (13.6%) | 1.000 |
| Altered sensorium | 1 (2.6%) | 1 (4.5%) | 1.000 |
| SOB | 2 (5.3%) | 0 (0.0%) | 0.528 |
| Renal symptoms | |||
| Anuria | 1 (2.6%) | 0 (0.0%) | 0.128 |
| Nonoliguria | 5 (13.2%) | 5 (22.7%) | |
| Nonoliguric AKI | 6 (15.8%) | 8 (36.4%) | |
| Oliguria | 26 (68.4%) | 9 (40.9%) | |
| Systolic BP | 119.47 ± 10.64 | 122.91 ± 10.49 | 0.231 |
| Diastolic BP | 76.32 ± 7.50 | 79.09 ± 8.11 | 0.185 |
| Latent time to referral | 7.13 ± 1.26 | 4.95 ± 1.49 | 0.0001* |
| Day stay | 6.82 ± 3.86 | 9.41 ± 6.80 | 0.113 |
| Total day | 13.96 ± 4.25 | 14.36 ± 7.09 | 0.810 |
| Serum creatinine at admission | 6.57 ± 2.49 | 6.02 ± 2.51 | 0.414 |
| Hemoglobin (g/dL) | 11.68 ± 1.77 | 11.23 ± 1.09 | 0.230 |
| Total leukocyte count | 11,834.21 ± 3902.89 | 9500.00 ± 2107.36 | 0.004* |
| Serum potassium | 4.26 ± 0.47 | 3.91 ± 0.51 | 0.009* |
| PH | 7.34 ± 0.07 | 7.35 ± 0.07 | 0.580 |
| Serum bicarbonate | 13.62 ± 4.59 | 14.99 ± 4.08 | 0.253 |
| pCO2 | 24.47 ± 4.87 | 26.19 ± 5.97 | 0.231 |
| pO2 | 79.89 ± 17.87 | 91.68 ± 14.06 | 0.010* |
| Total bilirubin | 4.20 ± 3.46 | 1.99 ± 1.86 | 0.002* |
| Direct bilirubin | 2.71 ± 2.23 | 1.15 ± 1.37 | 0.001* |
| SGOT | 97.39 ± 62.74 | 45.04 ± 33.50 | 0.0001* |
| SGPT | 105.05 ± 66.60 | 57.27 ± 62.99 | 0.008* |
| Alkaline phosphatase | 139.74 ± 64.24 | 144.23 ± 180.42 | 0.889 |
| Anion gap | 14.70 ± 4.76 | 16.87 ± 7.03 | 0.216 |
| Urine output | 518.42 ± 481.19 | 968.18 ± 450.80 | 0.001* |
| Duration of RRT | 3.79 ± 2.29 | 3.71 ± 2.00 | 0.900 |
| Type of RRT | |||
| HD | 35 (92.1%) | 17 (77.3%) | |
| HD and PD | 2 (5.3%) | 0 (0.0%) | |
| PD | 1 (2.6%) | 3 (13.6%) | |
| No RRT | 0 (0.0%) | 2 (9.1%) | |
| Other organ involvement | |||
| No organ involvement | 10 (26.3%) | 13 (59.1%) | 0.013* |
| Liver or Lungs (one organ) | 16 (42.1%) | 8 (36.4%) | |
| Liver + Lungs (two organ) | 12 (31.6%) | 1 (4.5%) | |
| Ventilator support | 23 (60.5%) | 15 (39.5%) | 0.0001* |
AKI, acute kidney injury; HD, hemodialysis; PD, peritoneal dialysis; RRT, renal replacement therapy; SOB, shortness of breath.
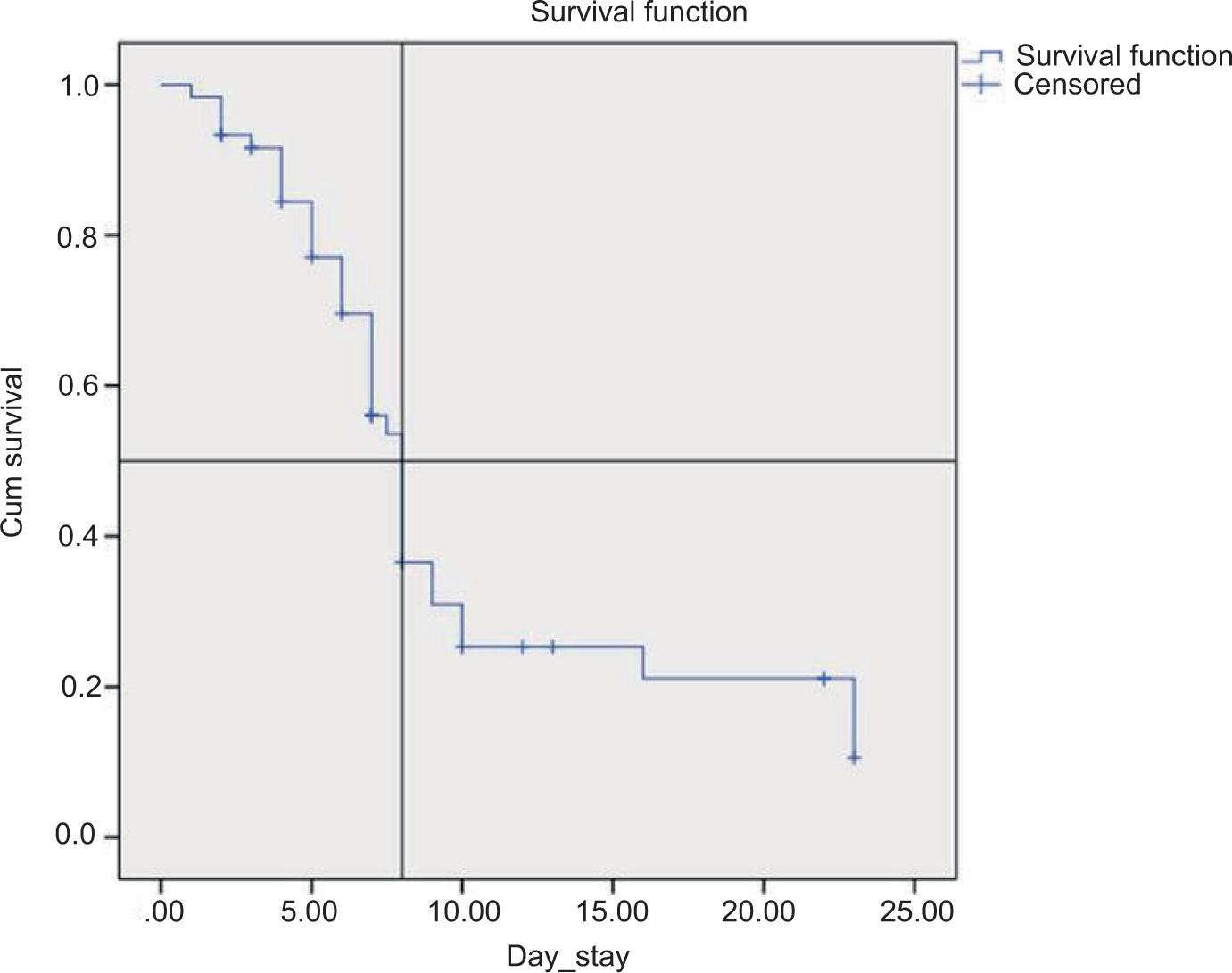
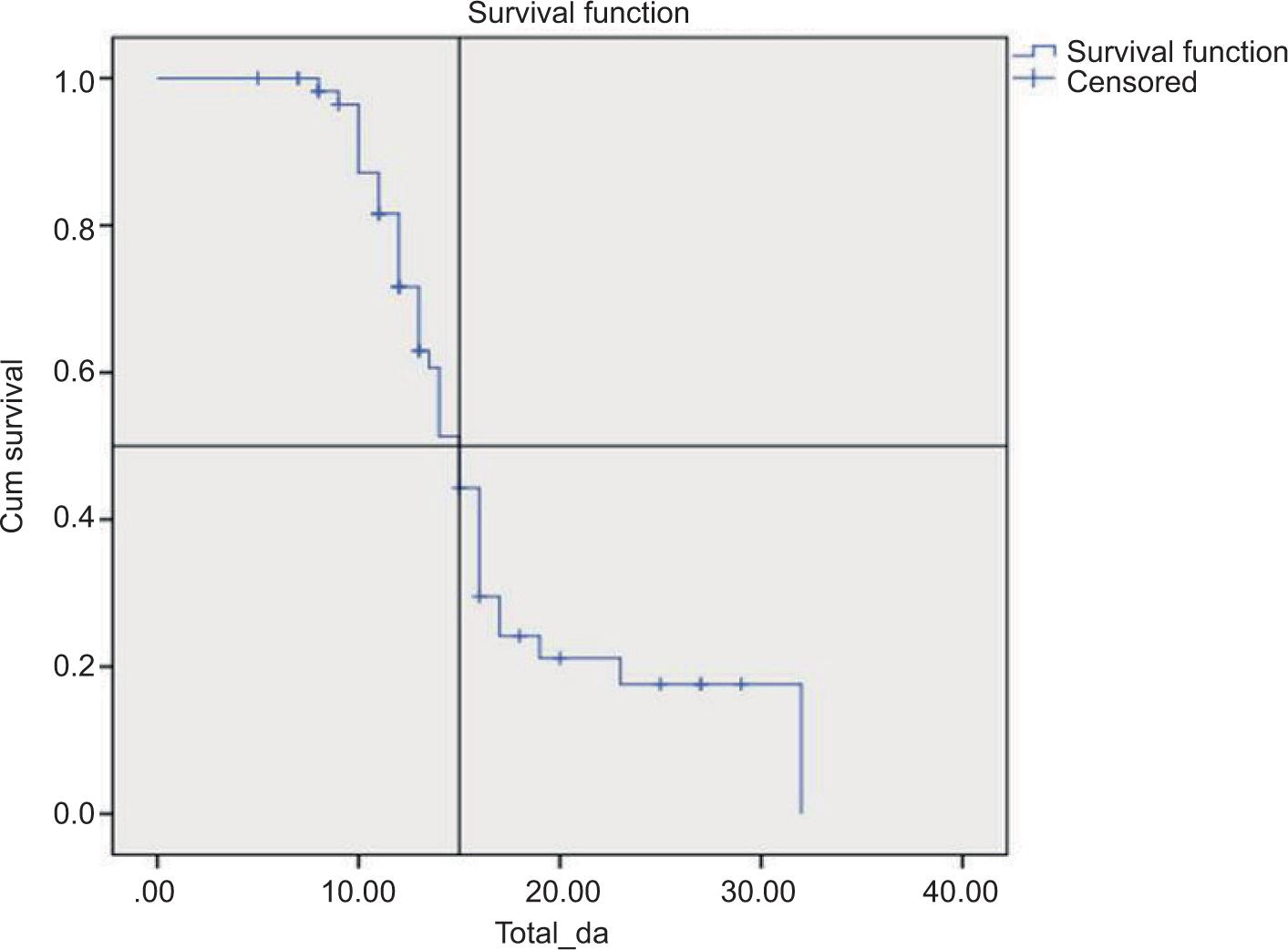
Further, survival analysis curves were predicted based on the data available. The probability of surviving 8 days was 50% in this group, and the probability of surviving 15 days in total period (latent period of referral + hospital stay) was 50%.
Discussion
Paraquat, or N, N'-dimethyl-4,4'-bipyridinium dichloride, also known as methyl viologen, is an organic compound with the chemical formula [(C–H–N)–]Cl–. It is an effective herbicide and weedicide and also an easily available suicide strategy. Failure of effective enforcement of various pesticide laws and regulations in the Indian subcontinent is the main cause of increasing suicides by pesticide consumption. Laxity in approach toward the use of paraquat for crops other than permitted crops is one of the main reasons for its easy availability in many Indian states. CIBRIC has approved the use of paraquat with a defined interval period for crops such as apple, tea, rice, cotton, maize, potato, and rubber (1). The main reasons for the increased use of paraquat in all crops are its easy availability, cost effectiveness compared to manual weeding, and efficacy as a weedicide (1). Paraquat is applied in fields by dispersion and spraying. Spraying is the most recommended and adapted method of application compared to dispersion, but the states such as Andhra Pradesh and Telangana use the dispersing method due to its convenience and other logistic issues (1). According to the WHO, paraquat belongs to the Class II hazard, which is highly toxic after ingestion. The minimum lethal dose of paraquat was reported to be 35 mg/kg (2). It was also reported by WHO that the factors influencing survival would include route and amount of ingestion (those who consumed <6 g of paraquat would survive), time of hospitalization, gastrointestinal absorption, intention of consumption, and concentration of paraquat in blood and urine (2).
Paraquat is commercially available as Gramoxon or Gramo, Kataar, or Milquat. Though it is cautioned as an occupational hazard that requires the use of personal protection equipments (PPE) during handling, the practical utility of PPE by farmers has been reported to be far less (1).
Routes of accidental or intentional exposure to paraquat are multitude, such as oral consumption, inhalational spray, eye splash, and direct skin contact. Irrespective of the routes of exposure, systemic toxicity is high as paraquat gets distributed in the tissues easily.
Paraquat is excreted through urine predominantly and small amounts through exhalation and in bile. Toxicity effects of paraquat may be systemic or local depending on the site of exposure, including skin burns, dermatitis, corneal ulcerations, and scarring of cornea. A myriad of clinical manifestations, such as vomiting, altered sensorium, oral ulceration, dysphagia, and dyspnea, have been reported in the study by Sandhu et al. (3). Other clinical manifestations included abdominal pain, diarrhea, and melena. In some patients, paraquat tongue (mucosal lesions in oral cavity) may be caused due to toxicity. In our group, oral ulcers (38.3%), vomiting (41.6%), abdominal pain (21.6%), and oliguria (26.6%) were the common symptoms due to consumption. Melena, breathlessness, and dysphagia were present in few patients.
The damage to the kidneys and lungs, the key target organs, usually occurred within 2–5 days of consumption. Ingestion of large amounts of concentrate of paraquat (>50 mL of 20% ion w/v) would lead to severe multiorgan failure causing pulmonary edema, AKI, acute hepatitis, and failure of the cardiac and nervous systems. Lung involvement occurs through various phases and can be in the form of alveolitis, alveolar collapse, pulmonary edema, and pulmonary fibrosis (4,5). It causes severe acute tubular necrosis in the kidneys, and in liver leads to mitochondrial damage and degranulation of smooth and rough endoplasmic reticula (6).
The severity of toxicity depends on the bioavailability of paraquat, as it gets distributed in a compartmental fashion. Due to this distribution pattern, the initial elimination half-life is around 6 h in initial phases but extends to 4 days after the first day of consumption. Hence, the methods such as hemadsorption would be effective in removal during the initial phases of bioavailability (within 2–4 h). In addition, paraquat is taken up against a marked concentration gradient into the pneumocytes, and the elimination from this compartment is slower than from others (7).
In our study, all patients with severe AKI were analyzed, and also the prevalence of severe AKI among the total paraquat poisoning cases. Mild elevations in creatinine were not referred to nephrology services by the internal medicine team. Hence, all patients included in our study were those with severe renal insufficiency. Those with prerenal failure and AKI Stages I and II were managed by the critical care and internal medicine teams. Oliguric AKI was present in about 26%. Mean serum creatinine in our group was 6.37 + 2.4 mg/dL. Of the 60 patients, 57 (0.95%) received an RRT, of whom 52 (86.6%) were supported with hemodialysis (HD) and 3 patients (5%) were given peritoneal dialysis (PD). Two more patients received hybrid treatment of HD and PD. Three patients did not receive RRT at all. Though hemoperfusion was suggested in those patients with duration of consumption <2 h, all our patients were referred late to our hospital. The primary decontamination and resuscitative measures were given at the local hospital before referral to us. A study by Hsu et al. in 207 patients with paraquat poisoning found that early hemoperfusion may reduce mortality, especially in those who received a pulse of methylprednisolone and cyclophosphamide (8).
This is the largest series of paraquat poisoning with severe AKI. Few case reports in the literature (9–12) reported of paraquat poisoning with AKI. A series of 103 patients with AKI due to paraquat poisoning was reported by Weng et al. (13), where patients with AKI were compared with those without AKI and number of patients who required HD. In this study, 24 patients with AKI required HD, while the remaining AKI patients (198) did not require one. In our study, 57 patients needed an RRT. The study by Kim et al. reported oliguric AKI in 10 out of 278 patients with paraquat poisoning (14), and in another report by Pavan et al., 6 patients had paraquat AKI with 50% mortality (15).
Mortality rates are reported to be high in paraquat poisoning with AKI due to the underlying severe inflammation, release of cytokines, and reactive oxygen species (16). In our study, mortality was noted in 38 patients (63.3%), and the factors which showed significant association on univariate analysis were amount of consumption, latency of referral, leukocytosis, liver dysfunction, hypoxemia, and need for ventilation. On Cox regression analysis, the factors found to be significant were the amount of consumption, vomiting, and presence of jaundice. The amount of consumption was high because paraquat was mixed with soft drinks or locally made toddy and consumed, hence the amount of consumption was about 100 mL in many patients although the actual amount of mix was only about 10–20 mL.
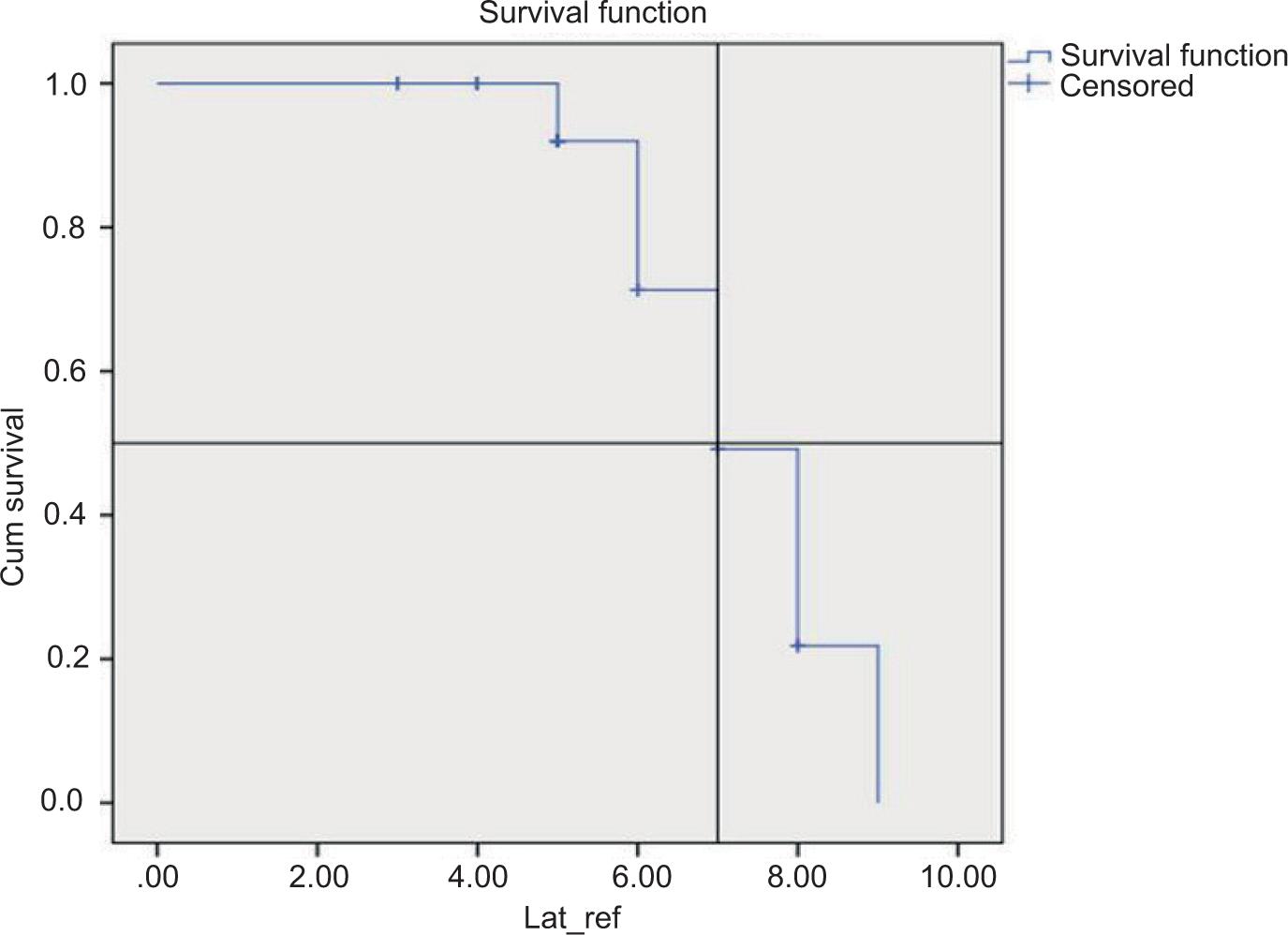
Survival analysis curves suggested a probability of 8-day survival after admission in 50%, and the probability of survival after the onset of consumption to be 15 days in 50%. This implies a high mortality rate in those with paraquat poisoning with severe AKI (Figures 1 and 2). Few studies have assessed the prevalence of severe AKI and the mortality among patients with paraquat ingestion as tabulated in Table 4.
Figure 1: The probability of surviving 8 days in hospital stay is 50%.
Figure 2: The probability of surviving 7 days in latent referral period is 50%.
Table 4: Cox-proportional hazard regression analysis.
| Characteristics | Univariate | Multivariate | ||
|---|---|---|---|---|
| Hazard ratio (95% CI) | P | Hazard ratio (95% CI) | P | |
| Age | 0.97 (0.93–1.01) | 0.141 | ||
| Consumption amount | 1.02 (1.01–1.04) | 0.0001* | 1.02 (1.01–1.03) | 0.001* |
| Sex | 1.07 (0.74–1.54) | 0.708 | ||
| Presenting symptoms | ||||
| Breathlessness | 0.97 (0.23–4.04) | 0.962 | 2.03 (1.05–3.91) | 0.035* |
| Abdominal pain | 0.63 (0.26–1.54) | 0.311 | 4.50 (1.28–15.85) | 0.019* |
| Oliguria | 1.41 (0.66–3.02) | 0.373 | ||
| Vomiting | 2.03 (1.06–3.90) | 0.034* | ||
| Icterus | 4.52 (1.30–15.68) | 0.017* | ||
| Oral ulcer | Figure | 0.136 | ||
| Melena | 0.57 (0.08–4.15) | 0.575 | ||
| Anuria | 5.56 (0.70–43.89) | 0.104 | ||
| Dysphagia | 0.68 (0.26–1.74) | 0.417 | ||
| Altered sensorium | 5.56 (0.70–43.89) | 0.104 | ||
| Breathlessness | 0.57 (0.08–4.21) | 0.581 | ||
| Systolic BP | 0.98 (0.95–1.02) | 0.50 | ||
| Diastolic BP | 0.95 (0.91–0.99) | 0.038* | ||
| Latent time to referral | 1.10 (0.89–1.36) | 0.362 | ||
| Day stay | 0.46 (0.36–0.59) | 0.0001* | 0.41 (0.30–0.55) | 0.0001* |
| Serum creatinine at admission | 0.98 (0.85–1.13) | 0.762 | ||
| Hemoglobin (g/dL) | 1.11 (0.91–1.37) | 0.303 | ||
| Serum potassium | 1.71 (0.93–3.15) | 0.084 | ||
| pH | 0.02 (0.00–2.63) | 0.114 | ||
| Serum bicarbonate | 0.98 (0.89–1.07) | 0.595 | ||
| pCO2 | 0.99 (0.93–1.07) | 0.975 | ||
| pO2 | 0.99 (0.97–1.00) | 0.163 | ||
| Total bilirubin | 1.18 (1.07–1.30) | 0.001* | ||
| Direct bilirubin | 1.26 (1.10–1.46) | 0.001* | ||
| SGOT | 1.01 (1.01–1.02) | 0.0001* | ||
| SGPT | 1.01 (1.01–1.02) | 0.0001* | ||
| Alkaline phosphatase | 1.01 (1.00–1.01) | 0.001* | ||
| Anion gap | 0.95 (0.88–1.02) | 0.162 | ||
| Urine output | 0.99 (0.99–1.00) | 0.034* | ||
| Duration of RRT | 0.72 (0.58–0.88) | 0.001* | ||
| Other organ involvement | 1.48 (0.99–2.21) | 0.056 | ||
| Ventilator support | 1.48 (0.76–2.87) | 0.250 | ||
*P-value significant.
RRT, renal replacement therapy; SGOT, glutamic-oxaloacetic transaminase; SGPT, serum glutamate pyruvate transaminase.
Figure 3: The probability of surviving 15 days in total period (latent period + hospital stay) is 50%.
In conclusion, we observed that the prevalence of severe AKI among paraquat poisoning is 4.5%, and the prevalence of severe AKI due to paraquat poisoning among all AKI cases admitted to nephrology services was 0.8% (60/6800 admissions). It was common in agricultural people, and the intention was suicidal in majority of the cases. The common symptoms of paraquat poisoning include oral ulcers, vomiting, and pain in the abdomen. The factors associated with mortality are amount of ingestion and latency of referral. The average expected survival in severe AKI due to paraquat was 8 days in 50% of the group.
Limitations
This is a retrospective study, and the dynamic evaluation of patients is not available.
A few markers of inflammation and the evaluation of degree of lung damage could not be assessed completely in all patients.
None of the survivors with nonrenal recovery underwent a renal biopsy.
Conflicts of Interest
None declared.
REFERENCES
1. Dileep Kumar D. Conditions of paraquat use in India [Internet]. Available from: https://www.iuf.org/wp-content/uploads/attachments/Joint%20paraquat%20study%20India_0.pdf
2. World Health Organization [Internet]. Paraquat and diquat. EHC 39: 1984; Available at: https://apps.who.int/iris/bitstream/handle/10665/37301/9241540994-eng.pdf
3. Sandhu JS, Dhiman A, Mahajan R, Sandhu P. Outcome of paraquat poisoning. Indian J Nephrol. 2003;13:64–8.
4. Smith P, Heath D, Kay JM. The pathogenesis and structure of paraquat-induced pulmonary fibrosis in rats. J Pathol. 1974 Oct;114(2):57–67. 10.1002/path.1711140202
5. Vijeyaratnam GS, Corrin B. Experimental paraquat poisoning: A histological and electron-optical study of the changes in the lung. J Pathol. 1971;103(2):123–9. 10.1002/path.1711030207
6. Matsumori H, Matsumoto T, Ishikawa H. Acute toxic effects of paraquat on ultrastructure of rat liver. Acta Pathol Jpn. 1984;34(3):507–18. 10.1111/j.1440-1827.1984.tb07579.x
7. Gawarammana IB, Buckley NA. Medical management of paraquat ingestion. Br J Clin Pharmacol. 2011;72(5):745–57. 10.1111/j.1365-2125.2011.04026.x
8. Hsu CW, Lin JL, Lin-Tan DT, Chen KH, Yen TH, Wu MS, et al. Early hemoperfusion may improve survival of severely paraquat-poisoned patients. PLoS One. 2012;7(10):e48397. 10.1371/journal.pone.0048397
9. Ito H. Silent acute renal impairment after low-dose paraquat ingestion. Case Rep Acute Med. 2019;2(2):31–4. 10.1159/000501648
10. Safaei Asl A, Dadashzadeh P. Acute kidney injury in patients with paraquat intoxication; a case report and review of the literature. J Renal Inj Prev. 2016;5(4):203–6. 10.15171/jrip.2016.43
11. Isha IT, Alam ZN, Shaha BK, Bari MS, Bari MZJ, Chowdhury FR. Paraquat induced acute kidney injury and lung fibrosis: A case report from Bangladesh. BMC Res Notes. 2018;11:344. 10.1186/s13104-018-3425-3
12. Adejumo OA, Akinbodewa AA, Olafisoye OJ, Afolabi ON. Acute kidney injury following paraquat poisoning: An uncommon cause of acute toxic nephropathy. J Med Trop. 2016;18(1):51–3. 10.4103/2276-7096.177828
13. Weng CH, Chen HH, Hu CC, Huang WH, Hsu CW, Fu JF, et al. Predictors of acute kidney injury after paraquat intoxication. Oncotarget. 2017;8(31):51345–54. 10.18632/oncotarget.17975
14. Kim S-J, Gil H-W, Yang J-O, Lee E-Y, Hong S-Y. The clinical features of acute kidney injury in patients with acute paraquat intoxication. Nephrol Dial Transplant. 2009;24(4):1226–32. 10.1093/ndt/gfn615
15. Pavan M. Acute kidney injury following paraquat poisoning in India. Iran J Kidney Dis. 2013;7(1):64–6.
16. Van Vleet TR, Schnellmann RG. Toxic nephropathy: Environmental chemicals. Semin Nephrol. 2003;23:500–8. 10.1016/S0270-9295(03)00094-9
17. Mohamed F, Buckley NA, Jayamanne S, Pickering JW, Peake P, Palangasinghe C, et al. Kidney damage biomarkers detect acute kidney injury but only functional markers predict mortality after paraquat ingestion. Toxicol Lett. 2015;237(2):140–50. 10.1016/j.toxlet.2015.06.008
18. Mohamed F, Endre Z, Jayamanne S, Pianta T, Peake P, Palangasinghe C, et al. Mechanisms underlying early rapid increases in creatinine in paraquat poisoning. PLoS One. 2015;10(3):e0122357. 10.1371/journal.pone.0122357
19. Kim SJ, Gil HW, Yang JO, Lee EY, Hong SY. The clinical features of acute kidney injury in patients with acute paraquat intoxication. Nephrol Dial Transplant. 2009;24(4):1226–32. 10.1093/ndt/gfn615