
Download
CI = end expiratory IVCD-end inspiratory IVCD end expiratory IVCD × 100 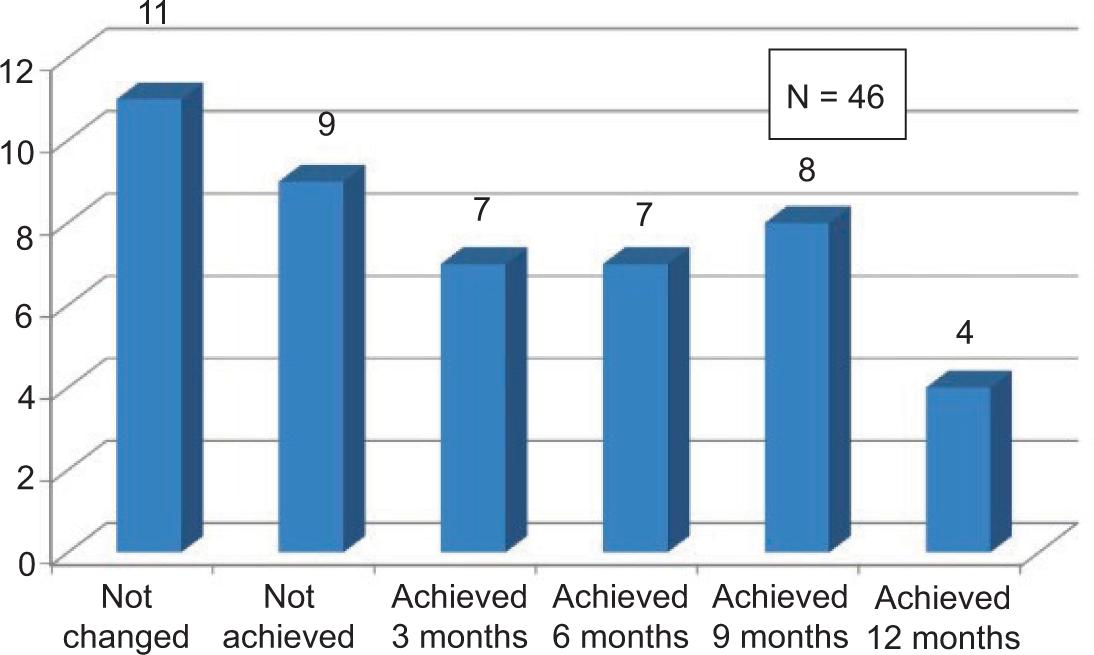
ORIGINAL ARTICLE: NEPHROLOGY
A Prospective Non-Randomised Interventional Study of Goal-Directed Ultrafiltration Compared With Clinical Dry-Weight Assessment in Achieving Euvolemic Status of Patients on Maintenance Hemodialysis
Pankaj Ganvir, C.H. Sudhiranjan Dash*, Amjad Khan Pathan, Rushi Deshpande, Ashay Shingare, Madan Mohan Bahadur, Ashwin Patil
Department of Nephrology, Jaslok Hospital and Research Center, Mumbai, India
Abstract
An accurate assessment of intravascular volume status in hemodialysis (HD) patients presents a significant challenge. Current clinical practices to determine dry weight is flawed due to interobserver variability and nonreproducibility. This miscalculation results in either chronic hypervolemia or hypovolemia with intra or interdialytic hypotension. The quest for noninvasive volume assessment tools to aid in the estimation of dry weight still continues. This study aims at goal-directed ultrafiltration removal compared with clinical dry-weight assessment in achieving euvolemic status of patients on chronic HD. It is a prospective, single-centered, nonrandomized, noninvasive interventional study on HD patients, for 12 months. Fifty two patients participated out of which 46 completed the study. Ultrasound-guided inferior vena cava collapsing index (IVCCI) and B lines were measured at intervals along with cardiac parameters. Dry weight was first estimated clinically by trial and error method. New dry weight target was set when B-lines were less than four in the eight site lung ultrasound and IVCCI between 50 and 75%, after 30 min post dialysis. Approximately 23.9% of the patients did not require dry-weight modification throughout the study. About 19% patients did not achieve dry weight in spite of all interventions. Overall, 56.5% of the patients achieved dry weight during the study period. A total of 46.3% of patients with NYHA Grade 3 dyspnoea observed at the start of study was reduced to 2.2%, showing statistical significance. Clinical assessment when bundled with noninvasive technology of assessment of dry weight showed encouraging results. B-lines and IVCCI estimation could be additional tools to achieve target weight goals, reducing complications and increasing compliance.
Key words: B-lines, dry weight assessment, hemodialysis, inferior vena cava collapsing index (IVCCI), left ventricular hypertrophy
Received: 9 June 2022; Accepted after Revision: 19 April 2023; Published: 3 July 2023
Author for correspondence: C.H. Sudhiranjan Dash, Department of Nephrology, Jaslok Hospital & Research centre, Mumbai, India. Email: sudhiranjan72@gmail.com
How to cite: Dash CHS, et al. A Prospective Non-Randomised Interventional Study of Goal-Directed Ultrafiltration Compared With Clinical Dry-Weight Assessment in Achieving Euvolemic Status of Patients on Maintenance Hemodialysis. J Ren Hepat Disord. 2023 7 (2): 1–9.
DOI: 10.15586/jrenhep.v7i2.148
Copyright: Dash CHS, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
An accurate assessment of intravascular volume status in hemodialysis (HD) patients presents a significant challenge. The quest for noninvasive volume assessment tools to aid in the reliable and reproducible estimate of dry weight still continues. Clinically, dry weight or the optimum post-dialysis weight is defined as the weight at which all or most of the excess body fluid is removed and below this threshold further fluid removal would produce unwanted side effects such as lethargy, feeling of prostration, hypotension, headache, and muscle cramps (1), while overestimation of dry weight may lead to hypertension, cardiac failure, oedema, and chronic fluids overload. Invasive methods such as central venous line insertion and monitoring of fluid status cannot be used routinely in chronic kidney disease (CKD) Stage 5D patients on HD.
Many methods exist to complete the clinical evaluation of the hydration status: cardiothoracic index based on chest X-ray evaluation, inferior vena cava (IVC) diameter evaluated by ultrasound, biomarkers such as brain natriuretic peptide, bio impedance spectroscopy (BIS), plasma volume variation monitoring (using crit-line monitor) (2), and lung ultrasound (3). Volume overload in patients on HD is an independent risk factor for cardiovascular mortality. B-lines detected on lung ultrasound (BLUS) assess the extravascular lung water. This raises interest in its utility for assessing volume status and cardiovascular outcomes, especially due to its noninvasiveness, free from radiation, ease of use, acceptable intra- or interoperator reproducibility, and limited interpersonal variability. With the easy availability of portable ultrasound devices in dialysis units, lung ultrasonography can be considered one of the most interesting “cards to play” for near-precise assessment of volume status in patients on maintenance HD (4). Lung ultrasound can evaluate extravascular lung water by identifying B-lines, which are vertical artefacts arising from the pleural line and extending to the edge of the screen that move synchronously with respiratory acts. Such artefacts arise from internal reverberation due to increase in fluid in lung lobes and segments. The reduction in the number of B-lines, on lung ultrasounds done before and after dialysis, confirms that these artefacts seen before dialysis are due to fluid overload.
Imaging studies of diameter of IVC can be used to assess intravascular volume in HD patients. Measurement of IVC diameter, respiratory variation with collapsibility, is observed to correlate well with central venous pressure. Collapsibility index (CI) can be calculated using the following formula (5):
Nonlinear regression analysis has confirmed that CI has a strong correlation with mean right atrial pressure, as assessed by cardiac catheterization (6). Kircher et al. reported similar results. He observed that CI > 50% was associated with lower right atrial (RA) pressure < 10 mmHg, whereas CI < 50% indicated raised RA pressures more than 10 mmHg (7).
CKD is an independent risk factor for cardiovascular disease, and as CKD progresses with time the complication rate increases (8). Cardiovascular (CV) mortality is 10–20 times more common in end-stage renal disease (ESRD) patients on renal replacement therapy as compared to general population. One of the major structural cardiac anomalies in patients with CKD is left ventricular hypertrophy (LVH), which is associated with increased risk of cardiac ischemia, congestive heart failure, and arrythmia. Majority of the patients with CKD die due to cardiovascular events before reaching ESRD due to both traditional and nontraditional risk factors. Whether CV events differ in patients with or without CKD is poorly defined, and whether the differences in cardiovascular outcomes could be mitigated with early prevention and change in therapeutic practices remain unclear in these population subset (4D trial) (9).
Hence, our study aims at goal-directed ultrafiltrate removal on the basis of IVCCI and B-lines on ultrasonography (USG) of chest in maintenance HD patients, which will lead to intradialytic and post-dialytic avoidance of complications due to hypovolemia or hypervolemia.
Materials and Methods
Study design
This was a prospective, nonrandomized, noninvasive interventional study. According to the reporting guidelines endorsed by the Consolidated Standards of Reporting Trials (CONSORT), this study is designed as per Strengthening of Observational Studies in Epidemiology (STROBE) statement.
Study duration
The duration of this study was 12 months from the first enrollment.
Study area
Patients on maintenance hemodialysis at the HD unit, Department of Nephrology, Jaslok Hospital and Research Center, Mumbai (single-center study).
Study population
Patients taking maintenance HD.
Inclusion criteria
All the patients who were taking maintenance HD for at least 6 months.
Exclusion criteria
Patients with one or more of these conditions who were undergoing HD, that is, decompensated cardiac failure, severe tricuspid regurgitation, pulmonary atrial hypertension, and septic shock.
Sample size calculation
Calculated by statistical software Open-Epi version for prospective study
Sample size, n = [Z2 P (1-P)]/d2 = 46 + 4.6 = 51 (approximate)
Where,
Z = Z statistic for a level of confidence,
P = expected prevalence, and
d = precision.
Explanation of sample size
In a previous study by Arun et al. (10), 43% of patients had favorable changes in their DW post intervention with a standard deviation of 93, confidence interval of 95%, margin of error = ±15%, and power of study as 95, and we get a sample size of 46. Considering a 10% dropout rate, we added 4.6 to 46. Hence, our final sample size was 51 patients (approximate) (Figure 1).
Figure 1: DW comparison – No. of patients who achieved DW, did not achieve DW, DW modification was not required.
Methodology
Written informed consent was taken from patients who were enrolled for the study. Patients enrolled in the study were advised to follow prescription of HD thrice per week with 4 h duration per session. B Braun Model Dialog plus evo and Fresenius 4008S dialysis machines were used for the HD sessions. Arteriovenous fistula and cuffed tunnelled HD catheter were used as access for HD. IVCCI, B lines, and NTproBNP were used as noninvasive tools for assessment of fluid volume status of patients. USG-guided assessment of IVCCI and B lines were done using Philips USG machine model Affinity 70G, by assigned radiologist at the bed side of the patient. As far as possible, the same radiologist service was sought after to limit the interobservability bias. In case the assigned radiologist was not available, opinions of two independent radiologists with agreeable values were taken. 2D ECHO was performed to assess LVH, EF, and diastolic dysfunction during the study period at Months 0, 3, and 6.
Dry-weight estimation of the enrolled patients was first done clinically (trial and error method). At the time of enrollment at Day 0 and during the run in phase of the first month, we considered those patients as our clinical standard dry weight control group. After 1 month, the same population served as the test population. At zeroth month, pre- and post-dialysis IVCCI and B-lines were checked. Again, post-dialysis B lines were checked at sixth and twelfth months. Post-dialysis IVCCI was assessed again at the third, nineth, and twelfth months. Every 3 months, the patient was assessed for symptoms related to volume depletion (cramps, orthostatic giddiness) and volume overload (breathlessness, edema). Any improvement or worsening in the quality of life was noted by standard questionnaires (feeling of breathlessness, weakness, requirement of extra session of HD, requirement of hospitalisation). Dry weight assessment was done every 3 months, and modification was done in those who were not achieving dry weight.
New dry weight in this study was defined as the weight of the patient at which the total number of B lines were <4. In the eight sites, LUS and IVCCI were between 50 and 75% on the integrated lung–IVC USG done 30 min post dialysis. Signs of fluid overload with blood pressure fluctuation status were studied. Need of extra session of HD apart from prescribed HD sessions or requirement of any hospitalization in between two HD sessions were noted. Dry weights of the enrolled patients were adjusted by modifying ultrafiltration volume by 10 mL/kg to attain the ultrasound-based criteria for dry weight.
The study was approved by Joint Ethics Committee and Basic Research Committee on July 25, 2018, Vide No. EC/988/2018.
Statistical analysis
-
After data collection, data entry was done in Excel sheet.
-
Data analysis was done with the help of SPSS software version 26.
-
Data was presented with the help of mean and standard deviation.
-
Qualitative data was presented with the help of frequency and percentage table.
-
Association among various study parameters were assessed by chi-squared test.
-
Pair student’s t-test was used to compare pre- and post values.
-
The significance threshold of P-value was set at < 0.05.
Results
A total of 52 patients were enrolled in the study of which 46 patients completed the study period of 12 months. Two patients underwent kidney transplantation, and four expired. Prior approval from the Institutional Ethics Committee Review Board was taken for study enrollment.
In our study, the mean age group was 57 years (Table 1) with the range varying from minimum 26 years to maximum 69 years, with patients between the age groups of 45 and 65 years contributing maximum (51.9%). In our study, 58% of the dialysis patients were males 42% were females. Diabetics represented about 73.1% of the total population along with hypertension in 75%. Out of the 52 patients, 67.3% had AV fistula and 32.7% patients had tunnelled HD catheter as HD access. Fifty-two patients were enrolled in the study, but only 46 patients completed the 1-year study duration. At zeroth month, pre-HD IVCCI > 50% was observed in 28.8% of the patients and post-HD IVCCI > 50% was observed in 59.6%. At twelfth month post-HD IVCCI > 50% was observed in 82.6% of the patients. This result was considered statistically significant (P < 0.05; Table 2). At the zeroth month, pre- and post-HD USG chest was done. About 69.2% of the patients had pre-HD B lines > 4 and post-HD B lines > 4 was observed in 38.5% of the patients. At twelfth month, post-HD B lines > 4 was observed in 17.4% of the patients. This result was considered statistically significant (P < 0.05; Table 3). Approximately 23.91% of the patients did not require dry-weight modification throughout the study as they fulfilled the revised DW criteria post intervention with maintenance of quality of life. Nineteen percent of the patients did not achieve dry weight in spite of all noninvasive interventions applied in the study. About 30.43% patients achieved dry weight within first 3 months, and 26.08% patients achieved dry weight in last 4 months of the study. Overall, 56.5% patients achieved dry weight during the study period. NYHA Grade 3 dyspnoea improved significantly in many patients by the end of the study. During the start of the study, there were 46.3% of patients with NYHA Grade 3 dyspnoea. As dry weight target was achieved, 2.2% of the patients had Grade 3 dyspnoea at 12 months. The result was considered significant (P < 0.007; Table 4). Grades 3–4 lower limb edema improved in our study group. Twenty patients had Grade 3–4 edema at the start of study. But by the end of the study, only one patient had Grade 3 edema and no patients with Grade 4 edema. There were 16 patients with Grade 2–1 edema at the start of study. But, by the end, 28 patients had grade 2–1 edema. Initially, 11.5% of the patients had intra HD cramps and giddiness; however, gradually the number of patients with cramps and giddiness increased to 20.4% at 6 months of study, but as expected at the end of study when dry weight was achieved, the number of patients with cramps decreased to 8.7%.
Table 1: Baseline characteristics.
| N | % | |
|---|---|---|
| Age distribution in years | ||
| ≤44 | 8 | 15.4 |
| 45–65 | 27 | 51.9 |
| >65 | 17 | 32.7 |
| Gender distribution | ||
| Male | 30 | 58 |
| Female | 22 | 42 |
| Access | ||
| AVF | 35 | 67.3 |
| Tunnelled catheter | 17 | 32.7 |
| Diabetes mellitus | 38 | 73.1 |
| Hypertension | 39 | 75 |
AVF, arteriovenous fistula.
Table 2: Month wise IVCCI (IVC collapsibility index) comparison.
| Month-wise no. of patients (%) | |||||
|---|---|---|---|---|---|
| IVCCI | Pre-HD 0 month (%) | Post-HD 0 month (%) | 3rd month (%) | 9th month (%) | 12th month (%) |
| < 50% | 37 (71.20) | 21 (40.2) | 25 (46.9) | 9 (19.6) | 8 (17.4) |
| > 50% | 15 (28.8) | 31 (59.6) | 27 (51.9) | 37 (80.4) | 38 (82.6) |
| Total No. | 52 | 52 | 52 | 46 | 46 |
This result was significant (P < 0.05), Higher the better.
HD, hemodialysis; IVCCI, inferior vena cava collapsing index.
Table 3: Month-wise B lines comparison.
| Month-wise no. of patients (%) | ||||
|---|---|---|---|---|
| B lines | Pre-HD 0 month | Post-HD 0 month | 6th month | 12th month |
| < 4 | 16 (30.8) | 32 (61.5) | 37 (75.5) | 38 (82.6) |
| > 4 | 36 (69.2) | 20 (38.5) | 12 (24.5) | 8 (17.4) |
| Total no. | 52 | 52 | 49 | 46 |
This result was significant (P < 0.05), lower the better. HD, hemodialysis.
Table 4: Month-wise comparison of dyspnea grading (NYHA).
| Month-wise no. of patients (%) | |||||
|---|---|---|---|---|---|
| Dyspnea grading | 0th month | 3rd month | 6th month | 9th month | 12th month |
| 1 | 19 (36.5) | 21 (40.4) | 22 (44.9) | 29 (63.0) | 30 (65.2) |
| 2 | 9 (17.3) | 11 (21.2) | 21 (42.9) | 16 (34.8) | 15 (32.6) |
| 3 | 24 (46.2) | 20 (38.5) | 6 (12.2) | 1 (2.2) | 1 (2.2) |
| Total no. | 52 | 52 | 49 | 46 | 46 |
This result was significant (P < 0.05).
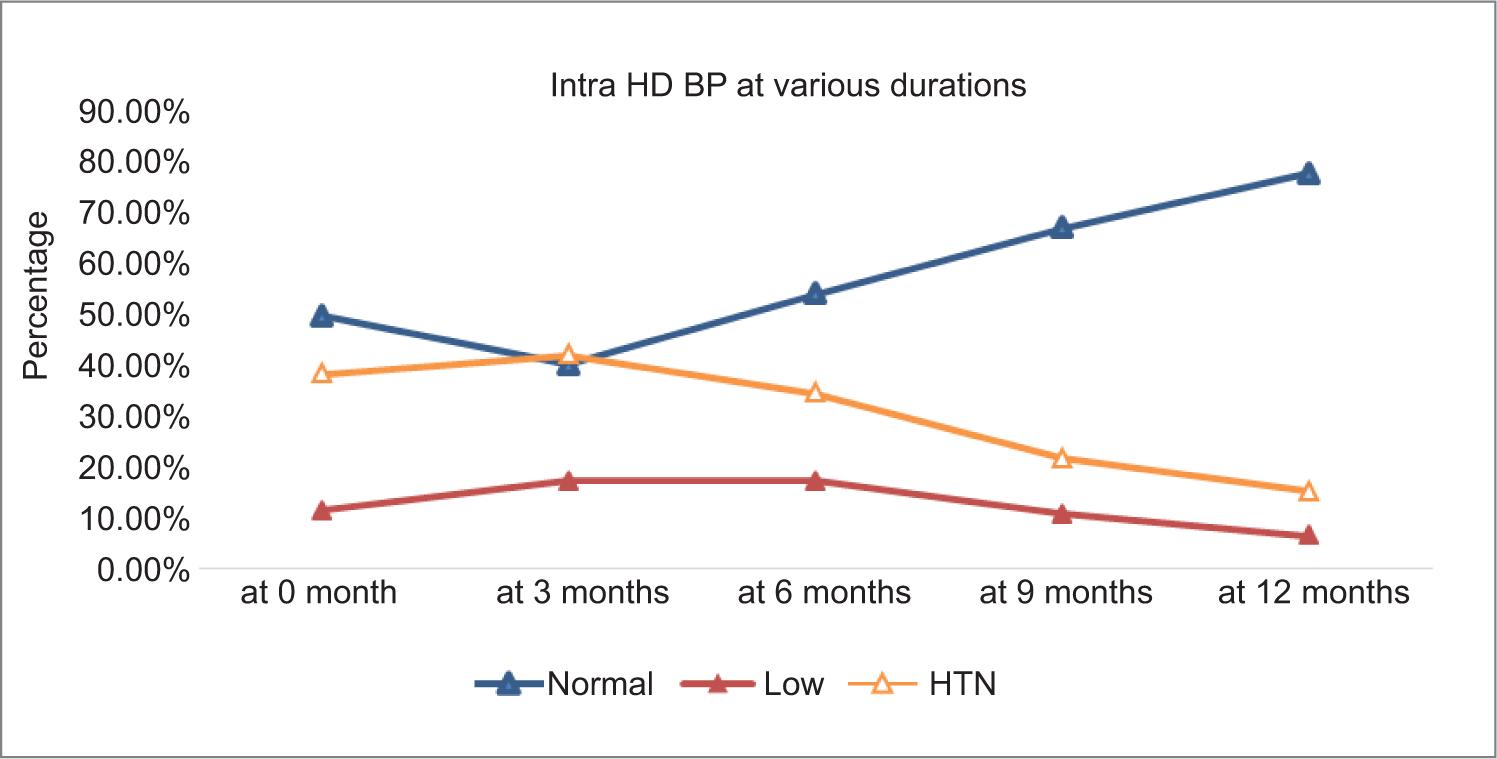
At months 0, 3, 6, 9, and 12, the proportions of patients having normal blood pressure were 26 (50%), 21 (40.4%), 25 (54.3%), 31 (67.4%), and 36 (78.3%), respectively. Similarly, the proportion of patients who had hypotension were 6 (11.5%), 6 (17.3%), 8 (17.4%), 5 (10.4%), and 3 (6.5%), respectively. The percentage of patients with hypertension during dialysis were 20 (38.5%), 22 (42.3%), 16 (34.8%), 10 (21.7%), and 7 (15.2%), respectively (Table 5).
Table 5: Intra-HD blood pressure.
| Time | Normal | Low | HTN | Total | |||
|---|---|---|---|---|---|---|---|
| At 0 month | 26 | 50.0% | 6 | 11.5% | 20 | 38.5% | 52 |
| At 3 months | 21 | 40.4% | 9 | 17.3% | 22 | 42.3% | 52 |
| At 6 months | 25 | 54.3% | 8 | 17.4% | 16 | 34.8% | 49 |
| At 9 months | 31 | 67.4% | 5 | 10.9% | 10 | 21.7% | 46 |
| At 12 months | 36 | 78.3% | 3 | 6.5% | 7 | 15.2% | 46 |
| Chi-square | 4.849 | 3.677 | 10.933 | ||||
| P | 0.303 | 0.451 | 0.027* | ||||
*significant at 5% level of significance; HD, hemodialysis; HTN, hypertension; NS, not significant.
Left ventricular ejection fraction (LVEF) did not worsen when compared initially and after 12 months. At the start of study, there were 19.2% patients with LVEF 50%. But by the end of the study, all patients who completed the study duration had LVEF 55–60%. The number of patients with LVEF 60% improved from 5.8 to 39.1%. LV thickness is assessed by calculating interventricular septal thickness (IVST) and left ventricular posterior wall thickness (LVPWT). Mean IVST and LVPWT did not change significantly, and so LV thickness is stable throughout the study without worsening. At the start of the study, mean IVST and LVPWT were 12.1 and 12.15, respectively. But by the end, the mean IVST and LVPWT were 11.7 and 11.9, respectively (Table 6). The percentage of cases with moderate diastolic dysfunction had increased from 3.8 to 43.5% when compared initially at the start of study and after 12 months. 7.7% of patients had severe diastolic dysfunction at the start of study, but by the end this decreased to 4.3%.
Table 6: Summary of variables with significance.
| Variables | At 0 month N = 52 Value |
95% CI | Pearson chi-square test | At 12 months N = 46 Value |
95% CI | Pearson chi-square test | P | |
|---|---|---|---|---|---|---|---|---|
| 1 | Breathlessness | _ | _ | _ | 2.143 | 1.462–3.141 | 13.084 | P < 0.007 |
| 2 | Cramps | 13.000 | 1.323–127.712 | _ | No -0.631 Yes-8.200 |
0.307–1.295 1.459–46.074 |
6.924 | |
| 3 | Giddiness | 13.000 | 1.323–127.712 | _ | No -0.631 Yes-8.200 |
0.307–1.295 1.459–46.074 |
6.924 | |
| 4 | Hypotension | _ | _ | _ | 1.636 | 1.13–2.36 | 22.601 | |
| 5 | IVCCI | 0.432 | 0.299–0.626 | 14.281 | 0.750 | 0.614–0.916 | 4.237 | P < 0.05 |
| 6 | B line | 2.250 | 1.562–3.242 | 14.444 | 1.320 | 1.088–1.601 | 3.815 | P < 0.05 |
| 7 | LVPWT | _ | _ | _ | 0.07 | 0.13–0.317 | 46.000 | P > 0.05 |
| 8 | IVST | _ | _ | _ | 0.237 | 0.163–0.641 | 41.592 | P > 0.05 |
IVCCI, inferior vena cava collapsing index; LVPWT, left ventricular posterior wall thickness; IVST, interventricular septal thickness.
Discussion
A total of 52 patents were enrolled in our study. The mean age of presentation was 57 years. Majority of the patients belonged to the age group 45–65 years (51.9%), and about 32.7% of the patients were above 65 years.
Studies done by Thomas et al., when compared with our study baseline characteristics, were found to be almost similar. In their study, maximum patients belonged to the age group of 40–59 years (62.2%), 25.7% were under the age group of 60–79 years, and 12.2% were under the age group of 18–39 years (10) . In our study, 67.3% of the patients used AV fistula and 32.7% had tunnelled dialysis catheter as an HD access. Most of the patients were dialysed with AV fistula (94.6%), and only 4.4% used tunnelled dialysis catheter in the study by Thomas et al. (10).
Our primary objective of ultrasound thorax–assisted dry weight calculation for each patient was performed at months 0, 6, and 12. At Month 0, pre- and post-HD USG chest in patients showed B lines > 4 in 69.2 and 38.5, respectively. However at twelfth month, we observed a significant reduction in post-HD B lines > 4 (17.4% of the patients), which showed a statistical significance (P < 0.05). Our study findings were concordant with the previous studies done by Tiba et al. and Basso et al. Hence, this study and the previous ones confirmed that USG lung-assisted dry weight assessment is superior to clinical assessment alone for detecting fluid overload (11).
In our study, IVCCI was estimated at different intervals during the study to look for fluid volume status. At zeroth month, pre- and post-HD IVCCI > 50% were observed in 28.8 and 59.6% of the patients, respectively. At twelfth month, post-HD IVCCI > 50% was observed in 82.6% of the patients. These results showed a significant P value < 0.007. It was observed that the majority of patients who were hypervolemic at baseline could achieve euvolemia at 12 months of study. The study by Thomas et al. (10) showed a significant improvement for pre- and post-HD differences in the measurement of IVC collapsibility index and number of B lines in lung ultrasonography.
In our study, 23.9% patients did not require dry-weight modification throughout the study. About 19% of the patients did not achieve dry weight in spite of all noninvasive interventions applied in the study. Approximately, 30.4% of the patients achieved dry weight within the first 3 months, while 26.1% achieved dry weight in last 4 months of the study. Overall, 56.5% of the patients achieved dry weight during the study period. So, B lines and IVCCI estimation helped in dry-weight achievement in 56.5% of the patients leading to their improvement in quality of life. The study by Noble et al. was the first to show that there was an association between ultrafiltration volume during HD and a subsequent change in B-line number, with a decrease of 2.7 B lines for every 500 mL of volume removed (12). The study by Enia et al. hypothesized that symptomatic and asymptomatic lung congestion contribute to poor physical performance in Stage 5 CKD patients on HD, and the number of ultrasound B lines were directly proportional to lower physical performance score (13). Our study did not include performance index assessment as an independent parameter, which could be a limitation. The study by Annamalai et al. showed a high correlation between absolute reduction of lung comet score and measured weight loss at the end of dialysis (14).
Instead, we included NYHA dyspnoea grades at different time periods to establish the quality of life. There were 46.3% of the patients with NYHA Grade 3 dyspnea at the beginning of the study, however at 12 months, only 2.2% had Grade 3 dyspnoea, which showed an improvement in parameter and showed a statistically significant value.
Intradialytic cramps and giddiness were noted in 11.5% of the patients at the start of study. We observed gradual increase in cramps and giddiness episodes to 20.4% at 6 months of study, but the number gradually decreased to 8.7% by the end of 12 months. As per the study by Annamalai et al., 12 out of 50 (24%) patients complained of cramps toward the end of dialysis. About 91% of these patients had no evidence of pulmonary congestion by lung ultrasound.
There was improvement in blood pressure control as the study progressed. Lung ultrasound and IVCCI gave an idea about ultrafiltration goal and hence prevented intradialytic blood pressure fluctuation. The proportion of study subjects with normal intra-HD blood pressure showed a slight increase, which was statistically insignificant (P = 0.303). Similarly, the proportion of study subjects with low intra-HD blood pressure showed a slight decrease, which was statistically insignificant (P = 0.451). However, the proportion of the study subjects with high intra-HD blood pressure showed a statistically significant decrease (P = 0.027). These results are shown in Figure 2. As per previous studies, reduction of volume overload was fundamental for blood pressure 9BP) control; and lung ultrasound–guided strategy for dry-weight reduction could effectively and safely control ambulatory BP values in HD population (15).
Figure 2: Intra HD BP at various durations.
LVEF and LVH did not worsen during the timeline of our study when compared at baseline and after 12 months of the study. In ESRD patients with systolic dysfunction, NHD leads to a sustained increase of EF and a reduction in the requirement for vasoactive medications in the absence of any reduction in post-dialysis extracellular fluid volume (16). Paradoxically, in this study, the percentage of cases with moderate diastolic dysfunction had increased from 3.8 to 43.5% when compared initially and after 12 months. 7.7% of the patients had severe diastolic dysfunction at the start of study, but by the end this reduced to 4.3%. Probable explanation for this observation could be in CKD Stage 5D patients with diabetes mellitus. It was observed that diabetic cardiomyopathy worsened with time, which could result in advanced LV diastolic dysfunction (17).
Heart failure with preserved ejection fraction (HFpEF) refers to a clinical syndrome in which patients have symptoms and signs of heart failure, normal or near-normal LV systolic function (ejection fraction [EF] over 50%), and evidence of diastolic dysfunction (DD), for example, abnormal LV filling and elevated filling pressure (18). This form of heart failure had become increasingly recognized and had a huge impact in CKD patients. As per Trinh et al., 60.4% of the patients had LVH regression or prevention at the end of 4.7 years follow-up (19). Our study was limited by a short follow-up period.
Conclusion
USG chest (B lines and IVCCI estimation) assisted with dry-weight assessment along with clinical assessment should be an additional noninvasive tool in achieving dry-weight goal. It not only reduces complication but also improves the quality of life in CKD Stage 5D patients on HD. Our study reinforces the above concept which was hypothesized by other studies. In this study, we could establish a statistically significant association of goal-directed ultrafiltration removal in achieving dry weight. Clinically asymptomatic lung congestion, a known entity in HD patients, could be detrimental in the long run. Hence, we propose the use of goal-directed parameters which will be better choice in reducing the complication rates. We could not establish the regression of LV thickness in the study period as it was too short to see the effect. However, we could establish the nonprogression of LV thickness at 12 months follow-up with improvement in diastolic dysfunction.
Some of the limitations of this study are as follows:
It was a nonrandomized study with a short follow-up duration. The performance index was not included as parameter in the study to show the improvement in quality of life.
Hard outcomes such as hospital admissions, cardiac events, all-cause mortality, or sudden cardiac death could not be evaluated as the sample size was too small and follow-up period was short to show a meaningful effect. Besides, this study design was not powered enough to evaluate the hard outcomes. Nevertheless, the study assumes importance given its noninvasiveness to determine the dry weight of HD patients in reducing complications.
Acknowledgment
We would like to extend our gratitude to Dr. Srinivas Desai, Head and Senior Consultant, Department of Radiology, Jaslok Hospital and Research Center, Mumbai for the support.
Disclosures
Funding for echocardiography and lung ultrasound was approved by the Institutional Basic Research Committee of JASLOK Hospital and Research Center, Mumbai.
Conflict of Interest
There are no conflicts of interest to disclose.
REFERENCES
1. Daugirdas JT, Blake PG, Ing TS. First Indian Reprint. 5th ed. Philadelphia, USA: Wolter Kluwer Heath; 2015. Handbook of Dialysis; pp. 205–6.
2. Arkouche W, Giaime P, Mercadal L. Les membres de la commission de dialyse de la Société de néphrologie. [Fluid overload and arterial hypertension in hemodialysis patients]. Nephrol Ther. 2013;9:408–15. 10.1016/j.nephro.2013.04.004
3. Allinovi M, Saleem MA, Burgess O, Armstrong C, Hayes W. Finding covert fluid: Methods for detecting volume overload in children on dialysis. Pediatr Nephrol Berl Ger. 2016;31:2327–35. 10.1007/s00467-016-3431-4
4. Di Nicolò P, Magnoni G, Granata. Lung ultrasound in hemodialysis: A card to be played. Blood Purif. 2017;44(1):1–7. 10.1159/000457897
5. Ilyas A, Ishtiaq W, Assad S, et al. Correlation of IVC diameter and collapsibility index with central venous pressure in the assessment of intravascular volume in critically Ill patients. Cureus. 2017;9(2):e1025. 10.7759/cureus.1025
6. Yildirimturk O, Tayyareci Y, Erdim R, Ozen E, Yurdakul S, Aytekin V, et al. Assessment of right atrial pressure using echocardiography and correlation with catheterization. J Clin Ultrasound. 2011;39(6):337–43. 10.1002/jcu.20837
7. Kircher BJ, Himelman RB, Schiller NB. Noninvasive estimation of right atrial pressure from the inspiratory collapse of the inferior vena cava. Am J Cardiol. 1990;66(4):493–6. 10.1016/0002-9149(90)90711-9
8. Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32(Suppl 3):S112–9. 10.1053/ajkd.1998.v32.pm9820470
9. Wanner C, Krane V, März W, Olschewski M, Asmus HG, Krämer W, et al. Randomized controlled trial on the efficacy and safety of atorvastatin in patients with type 2 diabetes on hemodialysis (4D study): Demographic and baseline characteristics. Kidney Blood Press Res. 2004;27(4):259–66. 10.1159/000080241
10. Arun Thomas ET, Mohandas MK, George J. Comparison between clinical judgment and integrated lung and inferior vena cava ultrasonography for dry weight estimation in hemodialysis patients. Hemodial Int. 2019;23(4):494–503. 10.1111/hdi.12762
11. Tiba MH, Belmont B, Heung M, Theyyunni N, Huang RD, Fung CM, et al. Dynamic limb bioimpedance and inferior vena cava ultrasound in patients undergoing hemodialysis. ASAIO J. 2016;62:463–9. 10.1097/MAT.0000000000000355
12. Noble VE, Murray AF, Capp R, Sylvia-Reardon MH, Steele DJR, Liteplo A. Ultrasound assessment for extravascular lung water in patients undergoing hemodialysis. Time course for resolution. Chest. 2009;135:1433–9. 10.1378/chest.08-1811
13. Enia G, Torino C, Panuccio V, Tripepi R, Postorino M, Aliotta R, et al. Asymptomatic pulmonary congestion and physical functioning in hemodialysis patients. Clin J Am Soc Nephrol. 2013;8(8):1343–8. doi:10.2215/CJN.11111012
14. Annamalai I, Balasubramaniam S, Fernando ME, Srinivasaprasad ND, Suren S, Thirumalvalavan K, et al. Volume assessment in hemodialysis: A comparison of present methods in clinical practice with sonographic lung comets. Indian J Nephrol. 2019; 29(2):102–10. 10.4103/ijn.IJN_78_18
15. Loutradis C, Sarafidis PA, Ekart R, Papadopoulos C, Sachpekidis V, Alexandrou ME, et al. The effect of dry-weight reduction guided by lung ultrasound on ambulatory blood pressure in hemodialysis patients: A randomized controlled trial. Kidney Int. 2019;95(6):1505–13. 10.1016/j.kint.2019.02.018
16. Chan C, Floras JS, Miller JA, Pierratos A. Improvement in ejection fraction by nocturnal haemodialysis in end-stage renal failure patients with coexisting heart failure. Nephrol Dial Transplant. 2002;17(8):1518–21. 10.1093/ndt/17.8.1518
17. Hung KC, Lee CH, Chen CC, Chu CC, Wang CY, Hsieh IC, et al. Advanced left ventricular diastolic dysfunction in uremic patients with type 2 diabetes on maintenance hemodialysis. Circ J. 2012;76(10):2380–5. 10.1253/circj.cj-12-0471
18. Pecoits-Filho R, Bucharles S, Barberato S. Diastolic heart failure in dialysis patients: Mechanisms, diagnostic approach, and treatment. Semin Dial. 2012;25:35–41. 10.1111/j.1525-139X.2011.01011.x
19. Trinh E, Chan CT. Intensive home hemodialysis results in regression of left ventricular hypertrophy and better clinical outcomes. Am J Nephrol. 2016;44(4):300–7. 10.1159/000449452