
Download
ORIGINAL ARTICLE: NEPHROLOGY
Impact of Induction Therapy on Clinical Outcomes of Kidney Transplant Recipients: A Single-Centre Cohort Study
Vijaya Madhuri Devraj, Gangadhar Taduri, Swarnalatha Guditi, Uttara Das, MP Shamsudheen, Megha Saigal, Raja Kartik Kalidindi*
Department of Nephrology, Nizam’s Institute of Medical Sciences, Punjagutta, Hyderabad, Telangana, India
Abstract
The purpose of this study was to evaluate long-term efficacy of immunosuppressive drugs based on the type of induction therapy given to kidney transplant recipients, and determine the occurrence of graft dysfunctions or rejections. We compared the safety and efficacy of anti-thymocyte globulin (ATG) and basiliximab (BAS) in high-risk patients and analyzed the cumulative incidence of immediate, slow, and delayed graft function in kidney transplant recipients to determine their initial short-term graft function. Evaluation of the long-term efficacy after 3 years post-transplantation by assessment of patients and graft survival, incidence of infections, and risks of rejection were the primary endpoints. Patients with stable graft survival were observed more with ATG (85%) than BAS (70%); in contrast, graft dysfunctions, graft nephrectomy, rejection episodes, and patient deaths were more prevalent with BAS than ATG, with statistically significant differences in long-term graft functioning. Patient survival at 3 years in ATG group was 90.4%, compared to 88% in BAS group, and graft survival was 90.4% in the ATG group and 81.3% in the BAS group (P < 0.001). The use of both induction therapies resulted in good patient and graft survival outcomes than placebo, and the results showed that there was a significant difference in both patient and graft survival after 3 years between induction of ATG and BAS, suggesting that ATG can be safer, effective, and preferable drug over BAS for high-risk recipients.
Key words: immunosuppressive therapy, induction therapy, initial graft function, long-term graft function, transplantation
Received: 13 December 2022. Accepted after Revision: 24 December 2022. Published: 24 January 2023
Author for correspondence: Raja Karthik Kalidindi, Department of Nephrology, Nizam’s Institute of Medical Sciences, Punjagutta, Hyderabad 500082, Telangana, India. Email: kalidindikarthik@gmail.com
How to cite: Devraj VM, et al. Impact of Induction Therapy on Clinical Outcomes of Kidney Transplant Recipients: A Single-Centre Cohort Study. J Ren Hepat Disord. 2023 7(1):1–10
DOI: 10.15586/jrenhep.v7i1.150
Copyright: Devraj VM, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
The success rate of transplantation depends on the administration of suitable immunosuppressive therapies. The main goal of immunosuppressive therapies is to induce tolerance by preventing loss of allograft without infection or toxicity and, most importantly, to achieve a long-term graft result.
After kidney transplantation, the immunosuppressive therapy usually involves induction therapy, followed by maintenance therapy. Initial induction with anti-lymphocyte agents is usually either through a T lymphocyte-depleting agent (Muromonab-CD3 mAb, alemtuzumab [anti-CD52 mAb] and polyclonal rabbit anti-thymocyte globulin [rATG]) or a non-lymphocyte-depleting agents interleukin-2 (IL-2) receptor antagonist (basiliximab [BAS] and daclizumab). Since the late 1990s, murine anti-CD3 monoclonal antibody muromonab-CD3 and horse ATG (eATG) are no longer used and daclizumab has been withdrawn, while polyclonal antibody rabbit ATG (rATG) and monoclonal antibody BAS are used more frequently (1).
Maintenance immunosuppressive agents consists of corticosteroids (prednisone and methylprednisolone), calcineurin inhibitors (cyclosporine and tacrolimus [TAC]), antiproliferative agents (mycophenolate mofetil [MMF], mycophenolate sodium, azathioprine, mammalian target of rapamycin inhibitors [everolimus and rapamycin/sirolimus]), and costimulation blockers (balatacept). A combination of a calcineurin inhibitor plus an antiproliferative drug, with or without corticosteroids, is usually used as a maintenance therapy. TAC and MMF have replaced cyclosporine and azathioprine, and they are being used in conjunction with low-dose corticosteroids (prednisone), thus reducing drug-related toxicity (2).
A series of trials have demonstrated that a combination of TAC, MMF, and prednisone has provided an effective immunosuppressive therapy resulting in fewer rejections (3). Hence, we focused on induction therapy. Many studies revealed that there was a clear association between induction immunosuppressive therapy on graft survival and outcome of kidney transplant patients with different immunological risks (4, 5). Induction therapy with ATG or interleukin 2 receptor subunit alpha (IL2RA) has been shown in a number of studies to minimize the probability of early acute rejection events after kidney transplantation, compared to controls (6, 7). Induction therapy often is increasingly utilized following kidney transplantation, although there is still a lot of debate/uncertainty about the benefits and hazards of using it as a part of modern post-transplant treatment. The choice of induction agent varies from place to place. In the United States, lymphocyte-depleting drugs, most commonly rATG, are currently utilized in 60% of kidney transplants, with IL2RA induction used in 20% of instances. On the other hand, in Europe IL2RA induction is more commonly used than rATG or other depleting drugs (8). According to Kidney Disease Improving Global Outcomes (KDIGO) guidelines, the use of lymphocyte-depleting drugs is advised only in patients with a high immunological risk (grade 2B). It is also believed that induction therapy helps in short-term graft survival, although its impact on long-term graft survival in renal transplant recipients has yet to be determined (9). Furthermore, there is no consensus on appropriate dosage and duration of treatment. Induction drugs at higher doses and for longer periods have been linked to an increased risk of infection, drug toxicity, and malignancies, while lesser doses may not be useful in preventing acute rejection (10). Hence, careful management of the recipient is still indispensable and requires drug combination to strengthen rejection prophylaxis and reduce doses of individual drugs in order to avoid toxic effects.
The aim of this study was to evaluate the efficacy and safety of polyclonal and monoclonal induction therapy with rATG and BAS on graft survival in kidney transplant patients with different immunological profiles in the present era of kidney transplantation. The study compared the group of patients according to the used induction (BAS vs. rATG) regarding the occurrence of acute rejection within the monitored period of 5 years after patients with standard immunologic risk had received transplants. In order to establish a risk-stratified strategy to induction therapy in kidney transplant recipients, we investigated the relationship between choice of induction therapy and outcomes following kidney transplantation.
Material and Method
Design
A total of 163 kidney transplant recipients who underwent transplantations between 2017 and 2021, and patients with higher immunological risks, were included in this retrospective cohort study with follow-up until January 2022. Induction therapy was based on perceived immunological risk; patients with higher immunological risk group were given ATG and BAS as induction therapy. Maintenance immunosuppressive regimen was common for all the patients. The study was designed to compare the clinical outcome of induction therapy. Patients were compared in two groups in accordance with their initial graft function (immediate vs. slow or delayed) and final graft function (stable graft function, graft dysfunction, graft nephrectomy, and patient deaths) along with other complications, such as incidence of rejections, infections, drug toxicity, new onset diabetes after transplant (NODAT), and hypertension (HTN).
Data collection
Donor and recipient characteristics, laboratory data, clinical data, and graft and patient survival status were retrieved retrospectively from medical records. We considered the following parameters:
-
Transplant-related variables included pre-transplantation medical and laboratory evaluation to assess medical suitability and adequacy of renal function based upon serum blood urea nitrogen, serum creatinine (Cr), and 24-h urine collection, levels of albumin, cholesterol, low-density lipoprotein, and high-sensitivity C-reactive protein. All immunological tests were performed to assess donor–recipient compatibility, such as human leukocyte antigen (HLA) typing, panel reactive antibody (PRA), donor-specific antibody test (DSA), complement-dependent cytotoxicity cross-match (CDC-XM), and T and B lymphocyte cross-match by flow cytometry based on clinical indications. Antibody specificity with a flow cytometry mean fluorescence intensity (MFI) thresholds of ≥1000 was considered positive.
-
Donor-related variables included a detailed medical, family, and social history questionnaire, such as age, gender, blood group, donor relation, donor type, number of matched HLAs, and cross-matching results. Cold ischemia time (CIT) and warm ischemia time (WIT) were also reviewed.
-
Recipient-related variables, such as age, gender, primary cause of kidney failure, native kidney disease (NKD), renal replacement therapy (RRT) type, dialysis modality and duration of hemodialysis (HD) vintage, type of transplantation, date of transplantation, and a history of pre-transplant issues, such as cardiopulmonary resuscitation, diabetes mellitus, hypertension, hepatitis C virus (HCV), induction and maintenance therapy, were reviewed.
-
Post-transplantation variables included post-transplantation issues, immediate graft biopsy, intervention provided, immediate graft function, HD sessions, day 4 TAC, baseline creatinine, discharge creatinine, post-transplantation rejections at time, type of rejection, post-transplantation infections, organism, cytopenia/leukopenia/pancytopenia, cytomegalovirus (CMV) infection, triple immunosuppressive modification, treatment outcome, other issues, and the final outcome.
Inclusion and exclusion criteria
Eligibility was determined according to the donor and recipient risk factors. High-risk recipients for acute rejections were required for eligibility. High immunological risk recipients were described as a recipients aged <18 and >60 years, dialyzing therapy for >3 years, highly sensitized recipients, such as loss of previous transplant secondary to rejection, blood group incompatibility, high number of HLA mismatches, PRA > 20%, presence of a DSA, cadaver donors, and longer cold ischemia time. Patients were excluded if they had undergone immunosuppressive therapy prior to transplantation, had recently taken an investigational drug, had a known allergic response to ATG or BSA, had a history of infection or were known to have hepatitis B surface antigen (HBsAg), hepatitis C virus (HCV), or human immunodeficiency virus (HIV), or had cancer (other than nonmelanoma skin cancer) during the previous 2 years. Women of childbearing potential who were not using oral contraceptives, nursing mothers, and pregnant women were also excluded.
Induction immunotherapy
Induction immunotherapy was delivered to high immunological risk patients, which were further divided into two groups. Immunotherapy induction with rATG (n = 40) or BAS (n = 77) was started in patients who had received cadaveric transplantation or those having a high risk of rejection. rATG was given intraoperatively after the patient was anesthetized at a dose of 1 mg/kg started as an infusion in 250-mL normal saline. The maximum dose being 80 mg, half dose was given before clamp release and rest of the dose given within 2 h of the first dose. Next dose was given on post-operative day 1 and the final dose on post-operative day 3. The patients were evaluated on a daily basis, because dose of rATG was administered based on the following parameters: lymphocytes > 300/mm3 and platelets > 5 × 104/mm3. If serious adverse effects, such as anaphylaxis, pulmonary edema, or viral infections, were discovered, rATG was temporarily stopped or interrupted. BAS was given at 20 mg on day 0 and day 4. On the other hand, for other non-high-risk cadaveric transplant patients and live-related renal transplant (LRRT) recipients, nondepleting agent BAS was given at 20 mg on day 0 and day 4. For lLRRTs, such as transplant from parent to children or among siblings who are HLA haplo/diplo matching, no induction therapy was prescribed, that is, control group (n = 46).
Maintenance immunosuppressive therapy
Maintenance immunosuppressive therapy included steroids, MMF (1200 mg per body surface area in two divided doses), and TAC (0.89 mg/kg/day) for all subjects. TAC levels were checked on post-operative day 4, and at the end of 1 month, 2, 3, and 4 months, and once stabilized, 6 months thereafter. Corresponding TAC trough concentrations were 15–20 ng/mL during the first 2 weeks; 10–15 ng/mL throughout week 3 and 4; 8–12 ng/mL during months 2 and 3; and 5–10 ng/mL thereafter. Azathioprine was started only if patient was having any severe adverse effects to MMF. The initial AZA dose was 2 mg/kg and adjusted according to adverse reactions. Initial prednisone dose was 0.5 mg/kg, with a maximum of 20 mg/kg during the first month, tapered slowly to 20 and 10 mg/kg during the second and third month, and ultimately 5 mg/kg on alternate days at the end of 1 year. Other prophylactic therapy given was valgancyclovir 450 mg on alternate days for 3–6 months, fluconazole 150 mg daily for 3 months, and trimethoprim and sulphamethaxizole, ½ tablet, daily for 3 months. Immunosuppression protocol was aimed to bring maintenance immunosuppression to the lowest dose by the end of 6-month period. Injection methyl prednisolone was prescribed to all patients as a pulse therapy at 1 gm/day for 3 consecutive days.
Short-term graft function
Initial graft function was generally detected by a drift in the patient’s serum Cr during the immediate postoperative period (POD) after induction therapy was specified in three groups based on clinical evaluation:
-
Immediate graft function (IGF)—this category comprised patients with normal renal function who recovered immediately post-transplantation with Cr < 3 mg/dL on post-operative day 5 (POD5); creatinine reduction ratio (CRR) of >20% for 3 consecutive days showed a fast recovery of renal function with satisfactory diuresis.
-
Delayed graft function (DGF)—these patients also showed decline in serum Cr from the base line but had Cr > 3 mg/dL on POD5 and CRR < 20% for 3 consecutive days; such patients required dialysis during the first post-transplant week.
-
Slow graft function (SGF)—such patients could be characterized by slower initial post-operative decline in serum Cr ≥ 3 mg/dL on POD5, and CRR < 20% for 3 consecutive days, with slow drop in renal function with an intermediate recovery of renal function with moderate diuresis, enough to avoid dialysis. Our primary outcome was to analyze initial graft function, for which we compared the incidence of IGF, SGF, DGF, and immediate graft loss (IGL) based on the type of induction therapy prescribed to renal transplant patients.
Long-term graft function
Kidney transplant recipients were analyzed for final outcomes of long-term graft function after 3 years; these were categorized into five groups: stable graft function, graft dysfunction, graft loss/graft nephrectomy, patient’s death, and lost follow-up. Patients with stable graft function, after transplantation had been maintaining normal serum creatinine and estimated glomerular filtration rate (eGFR) with no complaint. Patients with rise in serum creatinine of 15% from baseline were referred as graft dysfunction, which is often the primary indicator for biopsy, often associated with fever, graft tenderness, abnormal renal scan, and/or other clinical features commonly associated with an acute cell and/or antibody-mediated rejection reaction (AR). Obstruction, hypertension, or vascular stenosis, which failed to respond to high dose of triple immunosuppressive therapy, was associated with the sign of chronic rejection (CR). Decrease in renal function could be due to recurrence of infections (bacteria, fungal, or viral), NODAT, HTN, or calcineurin inhibitor (CNI) toxicity, which eventually causes acute tubular necrosis (ATN), focal and segmental glomerular sclerosis (FSGS), acute interstitial nephritis (AIN), pylonephritis (PN), and thrombotic microangiopathy (TMA) that ultimately lead to graft failure/loss or patient’s death (if not treated on time). Failure of renal allograft was defined as return to another form of renal replacement therapy (dialysis or re-transplantation). All suspected episodes of acute rejection were subjected to a graft biopsy, which was evaluated using the Banff 1997 criteria of allograft pathology. In case of clinical or laboratory evidence of graft dysfunction, duplex doppler ultrasound was performed. During episodes of DGF, biopsy was performed on weekly basis or 5–10-day intervals.
Statistical Analysis
Data analysis was performed by using the SPSS software, version 21. Data were presented as frequency tables, bar diagrams, and line graphs. Categorical variables were summarized as numbers n (%), Continuous data were presented as mean values and standard deviations (mean ± SD). For testing hypothesis, ANOVA t-test or Wilcoxon–Mann–Whitney test, Pearson’s Chi square test, and Kaplan–Meier method were used. t-test was used for comparison of two groups, and chi square (X2) test was used to check association between two or more attributed variables. Patient and graft survival analyses were determined using the Kaplan–Meier estimates and the log-rank test. P < 0.05 was considered statistically significant.
Results
Induction therapy
The present retrospective single-center cohort study evaluated long-term efficacy of induction therapy with ATG and BAS in renal transplant recipients. Of the 163 patients with high immunological risks according to KDIGO guidelines, 77 were randomly assigned to receive BAS, 40 received ATG, and the remaining patients who did not receive induction therapy were considered as the control group (n = 46). Comparisons between induction therapies given to recipients with respect to demographic details of donor and recipients, initial graft function, final graft function, rejections, infections, drug toxicity, and co-morbidities are listed in Table 1.
Table 1: Cumulative outcome measures of kidney transplant recipients on the basis of induction type; data are presented as mean ± SD or number (%).
| Variables of induction therapy | BAS (n = 77) |
ATG (n = 40) |
Control (n = 46) |
Total (n = 163) |
P-value | |
|---|---|---|---|---|---|---|
| Type of Tx | LRRT (n) | 21 | 8 | 46 | 75 | NS |
| DDRT (n) | 56 | 32 | 0 | 88 | ||
| Donor | Age (mean± D) | 37.89 ± 10.9 | 36.55 ± 10.5 | 37.75 ± 11.1 | 37.33 ± 10.8 | NS |
| CIT (hh.mm) | 3.89 ± 3.54 | 4.27 ± 3.97 | 3.66 ± 3.31 | 3.94 ± 3.60 | NS | |
| Recipient |
Age (mean±SD) | 32.84 ± 10.0 | 32.94 ± 9.8 | 32.67 ± 10.0 | 32.7 ± 9.9 | NS |
| Baseline serum Cr (mg/dL) | 1.5 ± 1.01 | 1.3 ± 0.36 | 1.2 ± 0.37 | 1.33 ± 0.58 | NS | |
| D4 TAC | 10.74 ± 2.06 | 10.03 ± 2.01 | 10.74 ± 2.11 | 10.38 ± 2.03 | NS | |
| Initial graft function | IGF | 41 (53.2) | 36 (90) | 43 (93.4) | 120 (73.6) | 0.002 |
| SGF | 14 (18.1) | 3 (7.5) | 1 (2.1) | 18 (11) | ||
| DGF | 19 (24.6) | 1 (2.5) | 1 (2.1) | 21 (12.8) | ||
| IGL | 3 (3.8) | 0 | 1 (2.1) | 4 (2.4) | ||
| Rejections | ABMR | 9 (11.6) | 3 (7.5) | 7 (15.2) | 19 (11.6) | 0.003 |
| TCMR | 1 (1.2) | 0 | 1 (2.1) | 2 (1.2) | ||
| Combined | 3 (3.8) | 1 (2.5) | 2 (4.3) | 6 (3.6) | ||
| Total rejections | 13 (16.8) | 4 (10) | 10 (21.7) | 27 (16.5) | ||
| Infections | Viral | 8 (10.3) | 4 (10) | 4 (8.6) | 16 (9.8) | 0.004 |
| Bacterial | 20 (26) | 7 (17.5) | 9 (19.5) | 36 (22) | ||
| Fungal | 8 (10.3) | 1 (2.5) | 0 | 9 (5.5) | ||
| Total infections | 36 (46.7) | 12 (30) | 13 (28.2) | 61 (37.4) | ||
| Drug toxicity | CNI/MMF | 5 (6.4) | 3 (7.5) | 7 (15.2%) | 15 (9.2) | NS |
| Comorbidities | NODAT | 15 (19.4) | 1 (2.5) | 2 (4.3%) | 18 (11) | NS |
| HTN | 5 (6.4) | 1 (2.5) | 1 (2.1%) | 7 (4.2) | NS | |
| Final graft function | Stable Graft function | 52 (67.5) | 32 (80) | 29 (63) | 113 (69.3) | 0.0006 |
| Graft dysfunction | 10 (12.9) | 4 (10) | 9 (19.5) | 23 (14.1) | ||
| Graft nephrectomy | 4 (5.1) | 0 | 3 (6.5) | 7 (4.2) | ||
| Patient death | 9 (11.6) | 2 (5) | 4 (8.6) | 15 (9.2) | ||
| Lost follow-up | 2 (2.5) | 2 (5) | 1 (2.1) | 5 (3) | ||
BAS, basiliximab; ATG, anti-thymocyte globulin; LRRT, living-related renal transplants; DDRT, deceased donor renal transplants; CIT, cold ischemia time ; SrCr, serum creatinine; Tac, tacrolimus; IGF, immediate graft function; SGF, slow graft function; DGF, delayed graft function; IGL, immediate graft loss; TCMR, T-cell mediated rejection; ABMR, antibody-mediated rejection; CNI, calcineurin inhibitors; MMF, mycophenolate mofeti; NODAT, new onset diabetes after transplant; HTN, hypertension; NS: non-significant values; P- value (*P < 0.05, **P < 0.005, ***P < 0.001).
Demographic details and clinical data
Demographic characteristics were similar in both groups. No significant differences in demographic features between both groups were observed with respect to age and etiology. Mean age of donors was 37.33 ± 10.8 years. Mean age of recipients was 32.7 ± 9.9 years. Mean time for cold ischemia was 3.94 ± 3.6 h. The mean follow-up period in the ATG group was 24.8 ± 10.8 months and that in the BAS group was 34.4 ± 10.5 months. The mean serum creatinine levels at the time of discharge were 1.5 ± 1.01 mg/dL and 1.3 ± 0.36 mg/dL in BAS and ATG groups, respectively, and 95% confidence interval for mean in the BAS group was (1.2105–1.7978) and that in the ATG group was (0.4043–2.1957). ANOVA was used for the comparison of BAS and the ATG groups. The significant calculated value was 0.485, which was insignificant at 5% level. Hence, we can say that there was no significant difference between both drugs concerning serum creatinine.
Short-term graft function
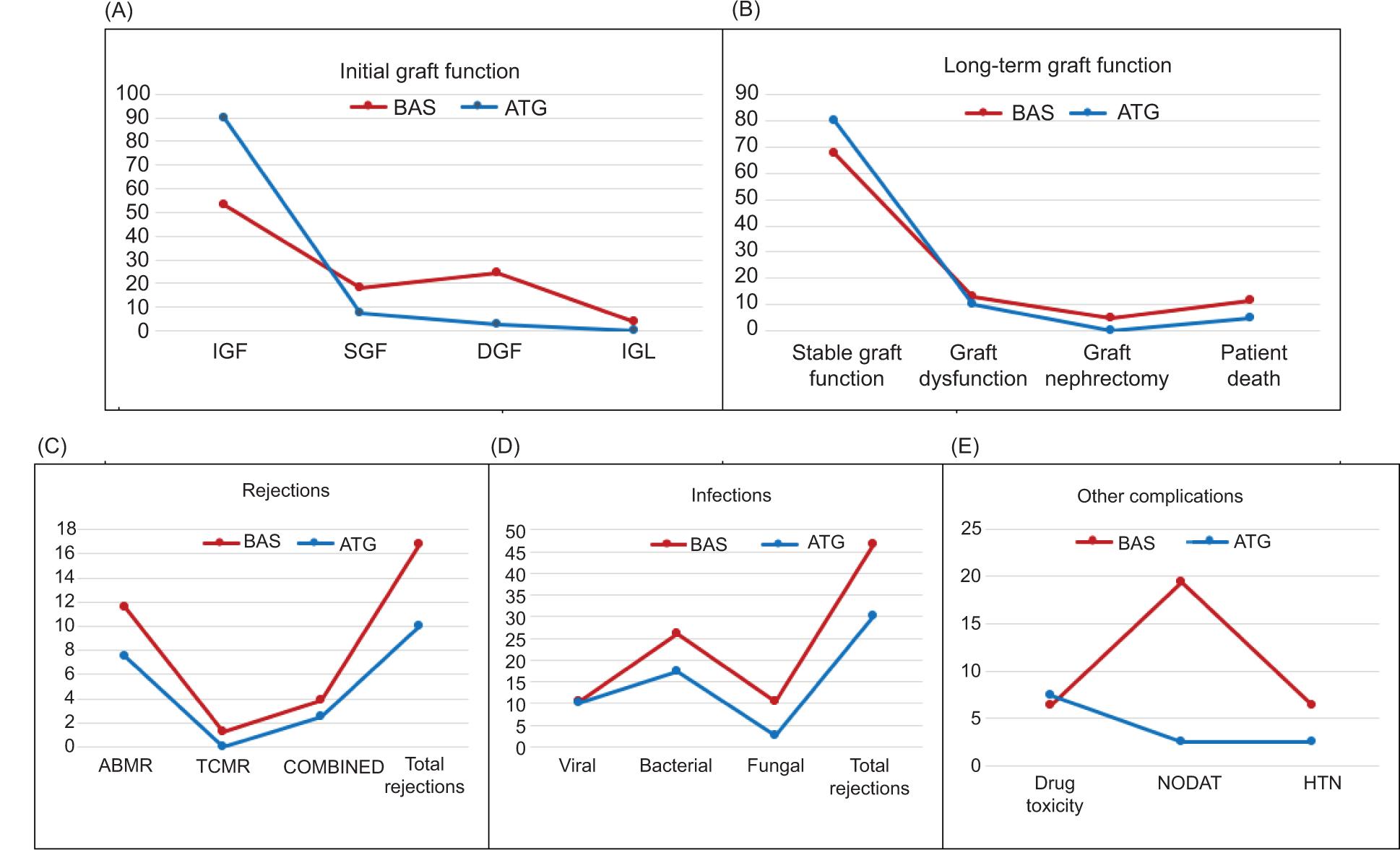
Our cohort of 163 transplants, initial graft function within one month from the date of transplantation was assessed based on cumulative incidences of IGF, SGF, DGF, and IGL. In all, 120 recipients (73.6%) experienced IGF; eighteen recipients (11%) SGF; 21 recipients (12.8%) DGF and four recipients (2.4%) IGL (Table 1). Immediate graft function IGF was found to be more with ATG (90%) than BAS (53.2%) group, while the incidence of SGF and DGF was observed more frequent among patients receiving BAS (18.1%, 24.6%) than ATG (7.5%, 2.5%), and IGL was found only in the BAS group (3.8%), but with no significant difference with the type of induction therapy given to the recipients (P = 0.07). However, comparison of these four groups showed statistically significant difference with the non-induction group (P = 0.002; Table 1 and Figure 1A).
Figure 1: Induction therapy with respect to (A) Initial graft function; (B) long-term graft function; (C) rejections; (D) infections; and (E) other complications.
Long-term graft function
Long-term graft function after 3 years from the date of transplantation was assessed based on the type of induction given to recipients. Out of 163 transplantations, 113 were stable graft function (69.3%), 23 were graft dysfunctions (14.1%), 7 were graft losses (4.2%), 15 deaths (9.2%), and 5 (3%) were lost in follow-up. Recipients with stable graft function were mostly observed with induction of ATG (80%), followed by BAS (67.5%), while graft dysfunction, graft loss, and patients’ death were found to be more with BAS (12.9%, 5.1%, and 11.6%, respectively) than ATG (10%, 0%, and 5%, respectively). Mortality was slightly higher in the BAS group, but the renal graft function improved rapidly in the ATG group, with statistically significant differences between both groups (P = 0.0008) and with the non-induction group (P = 0.0006; Table 1 and Figure 1B).
Rejections
In all, 27 (16.5%) biopsy-proven rejections were discovered. Rejections were more common in control group (21.7%), followed by 16.8% in BAS and 10% in ATG groups with statistically significant differences (P = 0.003). Comparative study between BAS and ATG demonstrated 11.6% antibody-mediated rejections (ABMR) in the BAS group and 7.5% in the ATG group; cellular-mediated rejections (TCMR) were only found in the BAS group (1.2%), while combined rejection was more with BAS (3.8%) than ATG (2.5%). The overall difference in the incidence and severity of rejections was significantly lower in the ATG group than in the BAS group (P = 0.05; Table 1 and Figure 1C).
Infections
Incidence of infection requiring hospitalization is shown in Table 1. In all, 61 (37.4%) patients experienced post-operative infections. Bacterial infection, such as urinary tract infection (UTI), tuberculosis (TB), diarrhea, drain-associated faecalis, pyelonephritis, epididymo-orchitis, occurred most commonly in 36 patients (22%). Sixteen patients (9.8%) encountered viral (CMV, polyomavirus [PMV], dengue, herpes zoster, and chicken pox) and 9 patients (5.5%) had fungal infection (fungal or cavitary pneumonia, and abscess). Higher prevalence of infection was found in the induction group than the non-induction group because of immunosuppressants with statistically significant differences (P = 0.004). Fungal infection in post-operative period was found to be more common in the BAS group (10.3%), followed by the ATG group (2.5%); however, viral was more in the BAS group (0.3%). Bacterial infection occurred at a significantly higher rate in the BAS group (26%) than in the ATG group (17.5%). This difference appeared to be attributable to a greater frequency of UTI. Although the incidents of overall infections were reported more in the BAS group (46.7%) than in the ATG group (30%), no significant difference was found between both groups (P = 0.333; Table1 and Figure 1D).
Other complications
Drug toxicity with CNI (TAC and cyclosporin) and MMF was found slightly higher in the ATG group (7.5%) than in the BAS group (6.4%) but with no significant difference (P = 0.504). NODAT or post-transplant diabetes mellitus was defined as the requirement of oral agents or insulin to control glucose concentration for more than 30 days. NODAT, unlike drug toxicity, was observed most commonly in the BAS group (19.4%) than in the ATG group (2.5%). Similarly, uncontrolled HTN was also higher in post-transplant patients of the BAS group (6.4%) than in the ATG group (2.5%) with no significant difference (P = 0.580). However, higher adverse effects were discovered in the BAS group (Table1 and Figure 1E).
Patient and graft survival
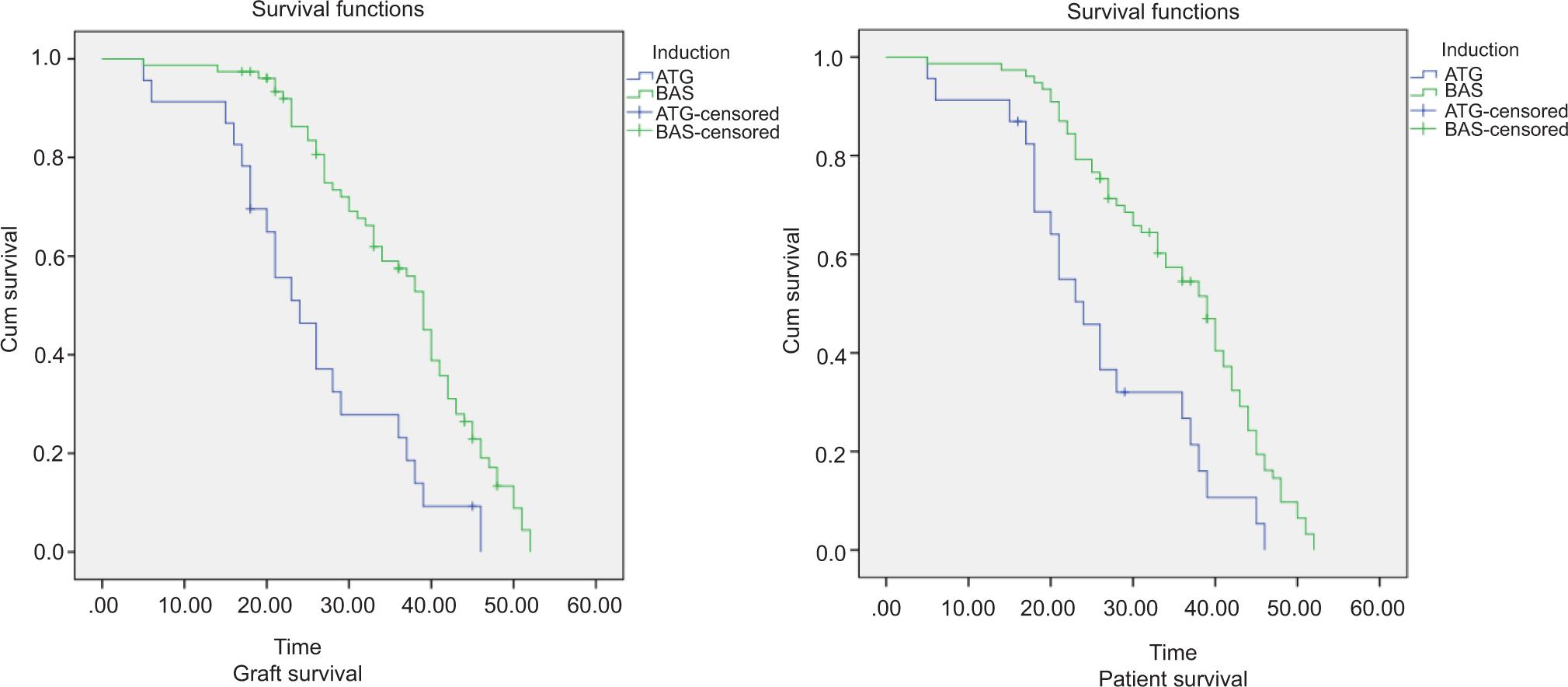
Patient survival rates after 3 years were 91.3% in the ATG group and 88.3% in the BAS group, and graft survival rate was 91.3% in the ATG group and 81.8% in the BAS group, with a statistically significant differences observed between the two groups using the Kaplan–Meier method (P = 0.001). In case of patients in whom transplant failure had not occurred, their time to event (transplant failure) was considered as censored at 60 months (Figure 2).
Figure 2: Patient and graft survival curve using the Kaplan–Meier method (P < 0.001).
Discussion
Induction therapy is administered before or immediately after transplantation to reduce the risk of early rejections so as to improve survival of the allograft. However, because of excessive immunosuppressive therapy, patients are at a higher of infectious difficulties. Yet, previous trials have confirmed that both ATG and BAS have a low risk of adverse effects and are safe, well-tolerated, and accepted. Currently, 60–80% of kidney transplant patients get ATG or BAS induction therapy, which has been demonstrated to minimize the severity of early post-transplant adverse effects.
Our study compared induction therapy with polyclonal antibody ATG and monoclonal antibody BAS in both short- and long-term survival. Initial graft function after transplantation has been shown to be a predictor of long-term transplant survival in many studies (11). According to our analysis, immediate graft function occurred most commonly in LRRTs. IGF occurred most commonly in LRRT, while SGF and DGF took place in cadaver transplants and have been found to be the cause for decreased rejection-free graft survival rates in high immunologically speculative patients. Induction therapy lowers the risk of DGF, although the administration of BAS intraoperatively did not reduce the incidence of DGF in this high-risk group but it lowered the severity and incidence of acute rejections. Hence, we found that the incidence SGF and DGF after transplantation early during post-transplantation period did not show much negative impact in achieving stable long-term outcome when ATG was used. Further, this has been linked to the decreased probability of acute rejection, and improved patient and graft survival in the long term. Although BAS and ATG were successful in delaying and lowering rejections, and thereby enhancing short-term life of graft, their impact on long-term survival of graft in renal transplant recipients has not been established thoroughly. As a result, the focus has been to long-term outcomes, with an emphasis on minimum rejections and other complexities. Among BAS and ATG, stable graft function was observed more with ATG. There was a trend toward a higher risk of graft dysfunction, graft nephrectomy, and patient deaths with BAS. Rejection rate and infections were also found to be more common with BAS. Although BAS is associated with a lower risk of drug toxicity than ATG, long-term outcomes do not appear to differ, and hence its influence on long-term graft survival remains inconclusive. Our results established that proportion of both patient and graft survival after induction with ATG and BAS were significantly different. ATG induction was associated with an improved trend in patient and graft survival. Nevertheless, CNI toxicity was reported to be marginally higher with ATG induction therapy but it had decreased incidence of rejections and infections, while BAS demonstrated slightly increased risk of post-transplant rejections. Infection rate and episodes of post-transplant complexities, such as NODAT and HTN, were more prevalent in the BAS induction group. However, statistically significant differences were not found between both groups, and the cause of higher rate of mortality in the BAS group could not be undetermined.
Different induction strategies were used at different centers to improve the outcome. Sandrini concluded that BAS helped in reducing DGF, hence it may be more preferable and safer for the induction therapy in patients of kidney transplantation (12). Our findings, however, argue against better graft survival with BAS than ATG, because in our study, the incidence of DGF occurred more in the BAS group and had higher incidence of rejections than in the ATG group. Similar to these results in many recent studies, ATG has exhibited superior results in avoiding acute cellular rejection in high-risk transplant patients (13). Studies conducted by Sailaja et al. and Seong et al. were a well-designed, randomized, controlled trial that compared ATG with BAS in high-risk patients (14, 15). The main findings in these studies were strikingly similar, as the rate of rejection was significantly lower with ATG than BAS, with no differences in patient and graft survival between the two therapies. Furthermore, study conducted by Patlolla discovered that lower rejection rate with ATG did not translate into better graft survival in the long term (16). Our study showed that ATG induction was associated with less rejection and improved patient and graft survival in the long term with statistically significant difference. Surprisingly, no trial has been conducted to compare ATG with placebo (17–20). We found that BAS showed a reduced rejection rate by 7%; however, ATG demonstrated a reduced rejection rate by 17% when compared with placebo, with improved graft survival.
It’s probable that cadaver donor type, donor’s age, and prolonged cold ischemia were associated with higher risk of rejection. However, we found that the effect of BAS and ATG on rate of rejection and graft survival was essentially the same in live versus cadaver donor transplants without any statistically significant difference. Although induction therapies in renal transplant recipients have been studied in the past, results of the present study demonstrated both short- and long-term outcomes.
In patients with low immunological risk, both ATG and BAS groups had similar 1-year rate of rejection, graft survival, and patient survival (21–23). However, recent studies conducted by Hannah et al. and Marta et al. confirmed that ATG is a more potent immunosuppressive agent than BAS but it does not seem to improve transplant survival and is likely to have an increased risk of infection (24, 25). These trials reported trends toward a statistically significantly higher incidence of CMV infection in the ATG group, compared with the BAS group. In contrast to these findings, our study indicated higher rate of infection with BAS but significantly decreased infections with ATG. The trend toward higher infections with ATG induction therapy was less striking. Hence, the superiority of ATG over BAS in preventing acute rejection without infection is undeniable. Furthermore, 3-year patient and graft survival was favorable in the ATG group. Hence, ATG can be considered as an efficient and safe induction agent.
There were several limitations to the present investigation. The sample size was small because this was a single-center trial, and the findings were inconsistent. Second, compared to 10–20 years, the graft function follow-up duration was short. The future research must thrust upon various parameters that influence graft survival, as the ultimate goal is to extend patient and graft longevity.
Conclusion
We confirmed in our analysis that patients with high immunological risks were benefited from rATG and BAS induction therapies, with less number of risk and complications than no induction group. Therefore, both induction regimens assured a safe and effective treatment and were associated with similar graft survival. Although short-term outcome in this trial did not show any significant difference between ATG and BAS groups, the long-term outcomes, including stable graft function, graft dysfunction, graft loss, and death rate, demonstrated a significant difference between the two groups. We observed that ATG reduced the severity of post-transplant adverse events, with the assumption of good graft functioning in the long-term post-transplant period. Hence, ATG could be more effective, efficient, safer, and preferable than BAS for relatively high immunological risk recipients with poor renal function in kidney transplantation.
Data Availability
The datasets analyzed in this study are not available publicly to protect patients’ privacy. Hence, any request to access the datasets should be directed to the corresponding author.
Author Contributions
VM Devraj and RK Kalidindi created the research design, collected material, and analyzed the data. G Taduri, S Guditi, RK Kalidindi, MP Shamsudheen and Megha Saigal performed the research. VM Devraj wrote the article, and G Taduri, S Guditi, and RK Kalidindi participated in the management and treatment of patients.
Conflict of Interest
The Authors declared no potential conflict of interest with respect to the research, finance, authorship, and/or publication of this article.
Ethics Statement
The study involving human participants was reviewed and approved by Institutional Ethical Committee of Nizam’s Institute of Medical Sciences.
Informed Consent
Written informed consent was taken from participants or legal guardians to participate in this study in accordance with national legislation and institutional requirements.
REFERENCES
1. Hardinger KL, Brennan DC, Klein CL. Selection of induction therapy in kidney transplantation. Transplant Int. 2013;26:662–72. 10.1111/tri.12043
2. National Kidney Foundation. New options in maintenance immunosuppression: A clinical update on managing kidney transplant recipients. New York, NY: National Kidney Foundation; 2015.
3. Phanish MK, Hull RP, Andrews PA, Popoola J, Kingdon EJ, MacPhee IAM et al. Immunological risk stratification and tailored minimisation of immunosuppression in renal transplant recipients. BMC Nephrol. 2020;21(1):92. 10.1186/s12882-020-01739-3
4. Marcus FL, Rodrigo SD, José AN, Raquel AF, Raquel GS, Evaldo N. Effects of immunotherapy induction on outcome and graft survival of kidney-transplanted patients with different immunological risk of rejection. BMC Nephrol. 2019;20(1):314. 10.1186/s12882-019-1497-5
5. Boucquemont J, Foucher Y, Masset C, Legendre C, Scemla A, Buron F et al. Induction therapy in kidney transplant recipients: Description of the practices according to the calendar period from the French multicentric DIVAT cohort. PLoS One. 2020;15(10):e0240929. 10.1371/journal.pone.0240929
6. Rita RA, Woodle ES, Abramowicz D, Dorry L, Castan R, Jilian NI et al. Rabbit anti-thymocyte globulin for the prevention of acute rejection in kidney transplantation. Am J Transplant. 2019;19:2252–61. 10.1111/ajt.15342
7. Maurizio S, Aris T. Immunosuppression in kidney transplantation. OBM Transplant. 2020:4(1):97. 10.21926/obm.transplant.2001097
8. Hellemans R, Bosmans JL, Abramowicz D. Induction therapy for kidney transplant recipients: Do we still need anti-IL2 receptor monoclonal antibodies? Am J Transplant. 2017;17:22–7. 10.1111/ajt.13884
9. Helfer MS, Pompeo JC, Costa ORS, Vicari AR, Ribeiro AR, Manfro RC. Long-term effects of delayed graft function duration on function and survival of deceased donor kidney transplants. Braz J Nephrol. 2019;41(2):231–41. 10.1590/2175-8239-jbn-2018-0065
10. Bayraktar A, Catma Y, Akyildiz A, Demir E, Bakkaloglu H, Ucar AR, et al. Infectious complications of induction therapies in kidney transplantation. Ann Transplant. 2019;24:412–7. 10.12659/AOT.915885
11. Rao C, Haifeng W, Lei S, Jianfei H, Jiawei P, Helong D et al. Predictors and one-year outcomes of patients with delayed graft function after deceased donor kidney transplantation. BMC Nephrol. 2020;21:526. 10.1186/s12882-020-02181-1
12. Sandrini S. Use of IL-2 receptor antagonists to reduce delayed graft function following renal transplantation: A review. Clin Transplant. 2005;19:705–10. 10.1111/j.1399-0012.2005.00417.x
13. Szczepanik A, Burrelli C, Bixby A, Yadav K, Chavin K. Basiliximab vs. antithymocyte globulin induction with early steroid withdrawal in kidney transplant recipients: Early rejection outcomes. Am J Transplant. 2020. https://atcmeetingabstracts.com/abstract/basiliximab-vs-antithymocyte-globulin-induction-with-early-steroid-withdrawal-in-kidney-transplant-recipients-early-rejection-outcomes/
14. Sailaja K, Purna P, Uma MR, Srinivasa MAR, Sahariah S. Anti-thymocyte globulin versus basiliximab induction in renal transplant recipients: Long-term outcome. Saudi J Kidney Dis Transpl. 2014;25:9–15. 10.4103/1319-2442.124459
15. Seong UC, Ju IM, Seok C, Se HY, Won MH, Sung RY. Comparison of the clinical outcomes between anti-thymocyte globulin and basiliximab induction therapy in deceased donor kidney transplantation: Single center experience. J Korean Soc Transplant. 2015;29:61–7. 10.4285/jkstn.2015.29.2.61
16. Patlolla V, Zhong X, Reed GW, Mandelbrot DA. Efficacy of anti-IL-2 receptor antibodies compared to no induction and to antilymphocyte antibodies in renal transplantation. Am J Transplant. 2007;7(7):1832–42. 10.1111/j.1600-6143.2007.01860.x
17. Boucquemont J, Foucher Y, Masset C, Legendre C, Scemla A, Buron F, et al. Induction therapy in kidney transplant recipients: Description of the practices according to the calendar period from the French multicentric DIVAT cohort. PLoS One. 2020;15(10):e0240929. 10.1371/journal.pone.0240929
18. Cristina D, Ramón C, Mireia C, Elizabeth P, Jose LL, Concepcion GG, et al. Low total dose of anti-human T-lymphocyte globulin (ATG) guarantees a good glomerular filtration rate after liver transplant in recipients with pretransplant renal dysfunction. Can J Gastroenterol Hepatol. 2018;2018:1672621. 10.1155/2018/1672621
19. Song T, Yin S, Li X, Jiang Y, Lin T. Thymoglobulin vs. ATG-Fresenius as induction therapy in kidney transplantation: A Bayesian network meta-analysis of randomized controlled trials. Front. Immunol. 2020;11:457. 10.3389/fimmu.2020.00457
20. Ko H, Min S, Han A, Mo H, Chung CTY, Kim HK, et al. Inferior outcomes of basiliximab compared to anti-thymocyte globulin induction therapy in kidney transplantation with weak pretransplant donor specific anti-hla antibody. Transplantation. 2020;104(3):366. 10.1097/01.tp.0000700404.96761.a6
21. Christophe M, Julie B, Claire G, Fanny B, Emmanuel M, Sophie G, et al. Induction therapy in elderly kidney transplant recipients with low immunological risk. Transplantation. 2020;104(3):613–22. 10.1097/TP.0000000000002804
22. Sang JK, Jinsoo R, Heejin Y, Kyunga K, Kyo WL, Jae BP. Outcome comparison between low-dose rabbit anti-thymocyte globulin and basiliximab in low-risk living donor kidney transplantation. J Clin Med. 2020;9(5):1320. 10.3390/jcm9051320
23. Lee H, Lee S, Jeon JS, Kwon SH, Noh H, Han DC, et al. Thymoglobulin versus basiliximab induction therapy in low-risk kidney transplant recipients: A single-center experience. Transplant. Proc. 2018;50:1285–8. 10.1016/j.transproceed.2018.02.088
24. Hannah K, Marta J, Mathieu H, Benjamin T, Ludovic DA, Pierre P, et al. Different impact of rATG induction on CMV infection risk in D+R-and R+ KTRs. J Infect Dis. 2019;220(5):761–71. 10.1093/infdis/jiz194
25. Marta J, Edoardo M, Elena C, Anna M, Nuria M, Joan T, et al. CMV-specific cell-mediated immunity at 3-month prophylaxis withdrawal discriminates D+/R+ kidney transplants at risk of late-onset CMV Infection regardless the type of induction therapy. Transplantation. 2018;102(11):e472–e480. 10.1097/TP.0000000000002421