
Download
K ru = UUN SUN × urine flow rate mL/min , Cr et = UV P ,
ORIGINAL ARTICLE: NEPHROLOGY
Quality of Life of Patients on Peritoneal Dialysis and Contributing Factors: A Cross-Sectional Study
Niloofar Nili1, Shiva Seirafian2, Sayed Mohsen Hosseini3, Abdolamir Atapour2, Maryam Kazemi Naeini1, Mojgan Mortazavi2*
1Isfahan University of Medical Sciences, Iran;
2Isfahan Kidney Diseases Research Center, Isfahan University of Medical Sciences, Iran;
3Department of Biostatistics and Epidemiology, Isfahan University of Medical Sciences, Iran
Abstract
In recent years, interest in Health-Related Quality of Life (HRQoL) as a major indicator of clinical efficacy and treatment outcome in patients of End-Stage Renal Disease (ESRD) has grown significantly. This study aimed to determine the contributing factors affecting the quality of life (QoL) of ESRD patients undergoing peritoneal dialysis (PD). A cross-sectional study was conducted on PD patients presented at PD centres of Al-Zahra and Noor hospitals in Isfahan, Iran, from May to August 2019. A total of 173 patients having peritoneal dialysis for more than 3 months filled the validated 36-item short-form health survey questionnaire (SF-36). Baseline demographic details and dialysis-related factors were collected from patients’ medical records. The overall QoL score of patients was 50.28 ± 20.87. Male patients had a higher QoL score than female patients (58.18 in males, compared to 48.18 in females; P = 0.04). A significant association between frequency of dialysis and quality of life was observed, where three sessions of dialysis per day yielded the highest quality of life (QoL score = 59.62; P = 0.047). A significant positive correlation was discovered between QoL score and residual renal function (P = 0.013). In addition, a higher QoL score was observed in self-employed patients (60.95), compared to housewives (46.49) (P = 0.001). QoL assessment should be included as an integral part of patient follow-up to evaluate treatment outcomes and implement possible interventions to improve patient’s quality of life.
Key words: chronic kidney disease, end-stage renal disease, peritoneal dialysis, quality of life, SF-36 questionnaire
Received: 12 October 2022. Accepted after Revision: 18 January 2023. Published: 1 March 2023
Author for correspondence: Mojgan Mortazavi, Department of Internal Medicine, Isfahan University of Medical Sciences, Iran. Email: m_mortazavi@med.mui.ac.ir
How to cite: Nili N, et al. Quality of Life of Patients on Peritoneal Dialysis and Contributing Factors: A Cross-Sectional Study. J Ren Hepat Disord. 2023 7(1):11–21
DOI: 10.15586/jrenhep.v7i1.151
Copyright: Nili N, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
Chronic kidney disease (CKD) and end-stage renal disease (ESRD) are major medical and public health problems worldwide and a serious challenge for many developing countries (1, 2). In Iran, like in other developing countries, diabetes mellitus and hypertension are the leading causes of ESRD. Other common causes of ESRD include glomerulonephritis, polycystic kidney disease, and obstructive uropathy (3–8). ESRD represents a progressive clinical condition in which an irreversible loss of endogenous renal function below a sufficient degree is established, imposing permanent dependency on renal replacement therapy (RRT) to avoid life-threatening uremia and other complications. Treatment of this disease is affected through RRT, including peritoneal dialysis (PD), hemodialysis (HD), or kidney transplantation (KT) (9–11).
Kidney transplantation has been accepted as the best RRT, contributing to the best prognosis, regarding either survival or quality of life in ESRD patients. However, owing to rapid increase in the prevalence of ESRD and the long waiting list for kidney transplantation, most patients with ESRD would go through a period of using any of the dialysis modalities in their life (12–15). It is a fact of clinical practice that while long-term survival is the center of attention of most physicians, ESRD patients care more about their health-related quality of life (HRQoL) and prefer to spend this time in satisfactory well-being, instead of achieving a longer life (16–19).
Quality of life (QoL) is a term that is difficult to define. It is both a subjective and multidimensional concept that is regarded as a useful indicator of individual’s well-being in both physical and mental aspects of health. According to the World Health Organization’s (WHO) definition of quality of life, it is individuals’ perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns (20–25).
In recent years, more attention has been focused on the psychological consequences of maintenance dialysis therapy in patients with ESRD, and interests in HRQoL as an evaluative factor of responsiveness and effectiveness of treatment has grown significantly. Hence, evaluation of outcomes of ESRD treatment has gone beyond traditional assessments, such as morbidity, mortality, and hospitalization rate, and HRQoL has been accepted as an important outcome measure from both clinician and patient perspectives (9, 24, 26–29).
Materials and Methods
Study design
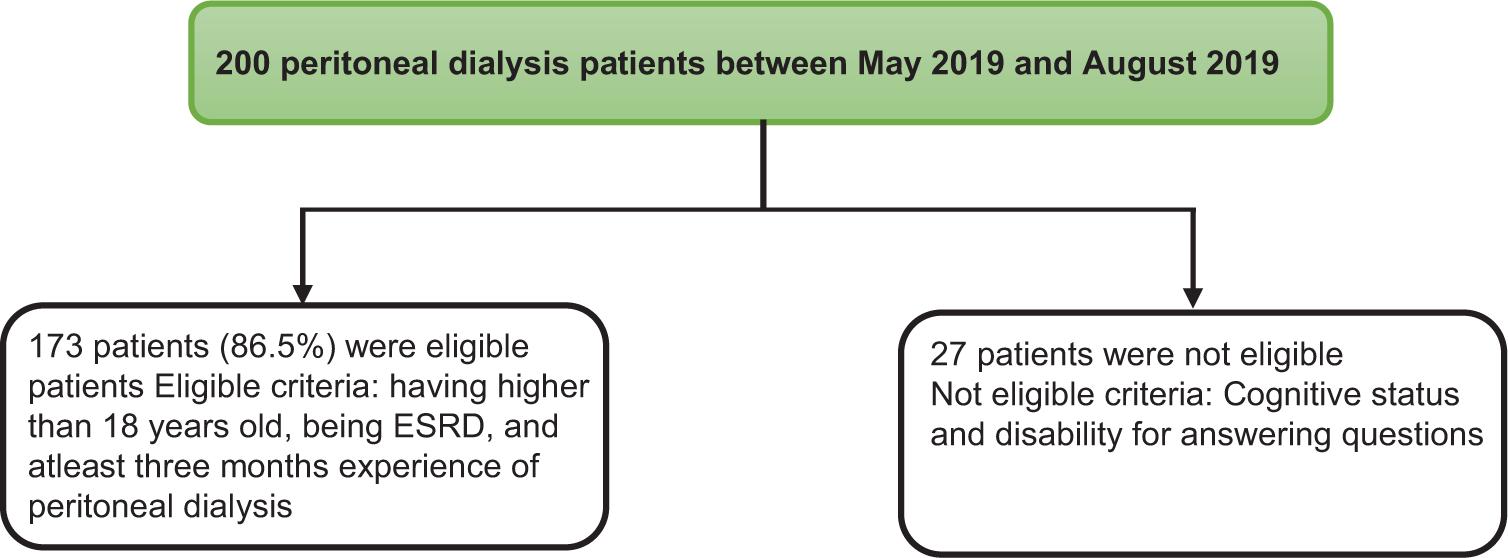
This cross-sectional study comprised ESRD patients undergoing peritoneal dialysis at the PD centers of Al-Zahra and Noor hospitals from May to August 2019. The inclusion criteria constituted patients aged more than 18 years, having ESRD, and undergoing peritoneal dialysis for at least 3 months. The exclusion criteria of the study included poor cognitive status and disability to answer questions (Figure 1). The entire study protocol was explained to all the patients having peritoneal dialysis at the centers for 3 months, that is, from May 2019 to August 2019. Written informed consent was obtained from all the patients for their anonymized information to be published in this paper. This study was approved by the ethical committee of the Isfahan University of Medical Science (IR.MUI.MED.REC.1398.425).
Figure 1: Study flow chart showing the inclusion and exclusion criteria of patients.
Variables included age, body mass index (BMI), gender, marital status, having separate room for peritoneal dialysis, employment, level of education, duration of the disease, comorbidities, duration of dialysis, type of solution used for peritoneal dialysis, and residual renal function (residual kidney clearance was approximated as the average of creatinine clearance [Krc] and urea clearance [Kru]). For calculating Kru, patient was required to collect complete urine of 24 h:
where UUN was the urine urea nitrogen concentration and SUN was serum urea nitrogen concentration.
Creatinine clearance (Crcl) was computed as the ratio of the per minute urine generation rate (from a 24-h urine collection) and the mean plasma level:
where UV = urine flow rate × urine creatinine concentration, and P was the mean plasma concentration of creatinine during the collection period.
Dialysis adequacy was calculated by the index of Kt/V. Peritoneal Kt/V was calculated by a 24-h collection of dialysate effluent and measuring its urea content. This was then divided by the average plasma urea level for the same 24-h period to give the clearance term, Kt. Residual renal Kt urea was calculated in the same manner using a 24-h collection of urine. Peritoneal and renal Kt results were then combined to arrive at total Kt per day, and divided by the estimated volume of distribution of urea using anthropometric equations for total body water (Watson’s equation).
Therefore, peritoneal Kt = daily drain volume × D/P urea,
renal urea clearance = renal Kt urea,
total Kt/V = peritoneal Kt/V + renal Kt/V,
V (by Watson’s equation) = 2.447 – 0.09516 A + 0.1704 H + 0.3362 W (in males),
V = –2.097 + 0.1069 H + 0.2466 W (in females),
where A = age (years), H = height (cm), and W = weight (kg) (30). Frequency of dialysis and hemoglobin levels were taken from patients’ medical records. In addition, patients were asked about their quality of life using a 36-item short-form health survey questionnaire (SF-36).
SF-36 Health Survey questionnaire
The SF-36 health survey questionnaire has a set of multi-purpose, generic, and easily administered quality-of-life measures. These measures are based upon patient’s self-reported status and are used for routine monitoring and assessment of treatment outcomes in adult patients. It consists of 36 items, which are divided into eight sub-scales: physical functioning (PF, 10 items), role physical (RP, four items), bodily pain (BP, two items), general health (GH, five items), vitality (VT, four items), social functioning (SF, two items), role emotional (RE, three items), and mental health (MH, five items). The scores of first four sub-scales are summed to create the physical composite score (PCS), while the scores of the last four sub-scales are summed to create the mental composite score (MCS). The format of questions is a combination of 5-point and 3-point scales, and dichotomous (yes/no) items. The higher total scores indicate a better HRQoL. The validity and reliability of the Persian’s version of SF-36 questionnaire was confirmed by Montazeri et al. in 2005 (31).
Statistical analysis
Qualitative variables were reported as frequency and frequency proportions, whereas quantitative variables were reported as mean values and standard deviation for normal variables and median and interquartile range for non-normal variables. The Kolmogorov–Smirnov test was used to assess the normality of variable distributions. To determine the correlation between QoL scores and other quantitative variables, Pearson and Spearman correlation tests were expended according to the normality of variables. To compare QoL scores and its sub-scales between different variables with two subgroups, independent Student’s t-test or Mann–Whitney U test was used. For variables with more than two subgroups, one-way ANOVA test with the Tukey post hoc test was used for normal variables and the Kruskal–Wallis nonparametric test for non-normal variables. Multivariable stepwise linear regression was used to investigate the simultaneous association of variables on QoL score. All statistical analyses were performed using Statistical Package for the Social Sciences 24.0 (SPSS Inc., Chicago, IL, USA). P < 0.05 was considered as statistically significant.
Results
The present study comprised 173 CKD patients who underwent peritoneal dialysis for at least 3 months. The characteristics of patients of the study are shown in Table 1. The mean age of the patients was 56.14 ± 16.55 years, 107 (61.8%) were males, and 130 (75.1%) patients were married. Most of the patients were housewives (34.9%), and the level of education of most of them was elementary (48%).
Table 1: Demographic and dialysis-associated characteristics of participants.
| Characteristics | Mean | SD | Count | Percentage | |
|---|---|---|---|---|---|
| Age (years) | 56.14 | 16.55 | – | – | |
| BMI (kg/m2) | 24.53 | 4.10 | – | – | |
| Gender | Male | – | – | 107 | 61.8 |
| Female | – | – | 66 | 38.2 | |
| Marital status | Single | – | – | 43 | 24.9 |
| Married | – | – | 130 | 75.1 | |
| Disease duration (months) | 109.71 | 99.9 | – | – | |
| Duration of dialysis (months) | 35.63 | 35.04 | – | – | |
| Dialysis adequacy | 1.91 | 0.48 | – | – | |
| Residual renal function (mL/min. 1.37m2) | 2.64 | 2.68 | – | – | |
| Hb (g/dL) | 11.07 | 2.06 | – | – | |
| QoL score | 50.28 | 20.87 | – | – | |
| Dialysis frequency (per day) | 1 or 2 | – | – | 14 | 8.2 |
| 3 | – | – | 68 | 39.8 | |
| 4 | – | – | 72 | 42.1 | |
| 5 or 6 | – | – | 17 | 9.9 | |
| Solution type | Solution 1 | – | – | 49 | 28.5 |
| Others (mix of icodextrin and conventional solution) | – | – | 123 | 71.5 | |
| Having separate room for peritoneal dialysis | Yes | – | – | 115 | 67.3 |
| No | – | – | 56 | 32.7 | |
| Employment | Housewife | – | – | 59 | 34.9 |
| Retired | – | – | 36 | 21.3 | |
| Self-employed | – | – | 52 | 30.8 | |
| Employee | – | – | 10 | 5.9 | |
| Unemployed | – | – | 7 | 4.1 | |
| Student | – | – | 5 | 3.0 | |
| Education | Ignorant | – | – | 30 | 17.3 |
| Elementary | – | – | 83 | 48.0 | |
| Diploma | – | – | 41 | 23.7 | |
| University | – | – | 19 | 11 | |
| Comorbidities | Diabetes mellitus | – | – | 11 | 6.4 |
| Kidney stone/cyst | – | – | 5 | 2.9 | |
| Diabetes mellitus + Hypertension | – | – | 51 | 29.5 | |
| Others | – | – | 103 | 59.5 | |
| Daily urinary volume (mL/day) | 471.47 | 539.09 |
The mean duration of kidney disease in all patients was 109.71 ± 99.9 months, and the mean duration of dialysis was 35.63 ± 35.04 months. The mean dialysis adequacy score was 1.91 ± 0.48, and their mean residual renal function was 2.64 ± 2.68. Most of the patients were dialyzed three (39.8%) or four (42.1%) times a day, and 115 (67.3%) of them had a separate room for dialysis at their home. Their mean hemoglobin level was 11.07 ± 2.06 g/dL. The most common comorbidity in the study participants was diabetes mellitus (35.9%). The overall QoL score of the participants was 50.28 ± 20.87 (Table 1).
Next, we assessed the association of demographic and dialysis-associated factors with QoL scores. Male patients had a higher QoL score, compared to female patients (58.18 [males] vs 48.18 [females]; P = 0.04). Considering the number of dialysis per day, a significant association was observed between frequency of dialysis and quality of life (P = 0.047), where three sessions of dialysis per day yielded the highest quality of life (QoL score = 59.62, P = 0.047). No statistically significant relationship was observed between quality of life and marital status, level of education, having comorbidities, solution type, or having a separate room for dialysis. As Table 1 shows, most of the patients were housewives. A higher QoL score in self-employed patients was ascertained, compared to housewives (60.95 [self-employed] vs 46.49 [housewives]; P = 0.001). In addition, no statistically significant association was discovered between QoL score and level of education (P = 0.36; Table 2).
Table 2: Difference in quality of life according to their contributing factors.
| Variable | QoL score | P* | |
|---|---|---|---|
| Gender | Male | 58.18 (19.84) | 0.04 (independent Student’s t-test) |
| Female | 48.18 (21.15) | ||
| Marital status | Married | 55.64 (20.48) | 0.157 (independent Student’s t-test) |
| Single | 50.048 (21.78) | ||
| Dialysis frequency | 1 or 2 | 54.95 (21.49) | 0.047 (ANOVA–Tukey post hoc test) |
| 3 | 59.62 (20.04) | ||
| 4 | 51.69 (21.14) | ||
| 5 or 6 | 45.30 (18.69) | ||
| Having a separate room for dialysis | Yes | 56.15 (22.10) | 0.086 (Mann–Whitney test) |
| No | 50.53 (18.29) | ||
| Employment | Housewife | 46.49 (20.11) | 0.001(ANOVA) |
| Retired | 58.45 (21.59) | ||
| Employed | 60.95 (18.49) | ||
| Education | Ignorant | 48.17 (20.72) | 0.36 (ANOVA) |
| Elementary | 56.27 (20.16) | ||
| Diploma | 54.74 (24.05) | ||
| University | 55.38 (17.11) | ||
| Education | Ignorant | 48.17 (20.72) | 0.36 (ANOVA) |
| Elementary | 56.27 (20.16) | ||
| Diploma | 54.74 (24.05) | ||
| University | 55.38 (17.11) | ||
| Education | Ignorant | 48.17 (20.72) | 0.36 (ANOVA) |
| Elementary | 56.27 (20.16) | ||
| Diploma | 54.74 (24.05) | ||
| University | 55.38 (17.11) | ||
| Comorbidities | Diabetes mellitus | 48.02 (23.96) | 0.67 (ANOVA) |
| Solution type | Diabetes mellitus + hypertension | 54.79 (21.49) | 0.184 (Independent Student’s t-test) |
| Others | 54.76 (21.49) | ||
| 1 | 57.99 (18.31) | ||
| Others (mix of icodextrin and conventional solution) | 52.81 (21.65) |
*Considered significant at P < 0.05.
As presented in Table 3, no statistically significant relationship was determined between the QoL score in peritoneal dialysis patients and age, BMI, hemoglobin level, disease duration, dialysis duration, and dialysis adequacy. Although residual renal function was associated with QoL scores in patients undergoing peritoneal dialysis (P = 0.013), a correlation coefficient of 0.230 accorded with a weak direct correlation between them (Table 3).
Table 3: Correlation between the QoL scores and contributing variables (Pearson and Spearman correlation).
| Quality of life | Age | BMI | Dialysis adequacy | Disease duration | Hb | Duration of dialysis | Residual renal function |
|---|---|---|---|---|---|---|---|
| Correlation coefficient | –0.089 | –0.040 | 0.095 | –0.123 | 0.103 | –0.031 | 0.230* |
| P-value | 0.279 | 0.628 | 0.248 | 0.139 | 0.208 | 0.712 | 0.013* |
| N | 151 | 151 | 150 | 145 | 151 | 148 | 115 |
Next, controlling the effects of gender, age, and BMI, we investigated the association of dialysis-associated variables with QoL score. Only residual renal function significantly associated with QoL scores (regression coefficient = 2.17 (0.71, 3.64, P = 0.046). No other variables showed any significant association with QoL scores.
Next, we assessed the association of contributing factors with SF-36 questionnaire sub-scales, including physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. Males and females were different in physical functioning, and males had a higher score (70 [males] vs 55 [females]; P = 0.010), they also had a better score for role physical (50 [males] vs 0 [females]), bodily pain (87.5 [males] vs 77.5 [females]), general health (50 [males] vs 40 [females]), and role emotional (66.66 [males] vs 0 [females]). However, marriage was not shown to be significantly associated with any of the sub-scales. BMI of patients also showed no significant association with any of the sub-scales. A significant association was found between age and physical functioning (P< 0.001). In addition, no significant association was discovered between comorbidities and any of the sub-scales. Self-employed patients yielded a better function in most of the domains, compared with housewives, and showed a better physical functioning (69.9 [self-employed] vs 49.71 [housewives], P = 0.003), role physical (75 [self-employed] vs 0 [housewives], P = 0 < 001), general health (54.18 [self-employed] vs 44.23 [housewives], P = 0.014), role emotional (66.66 [self-employed] vs 0 [housewives], P = 0.007), mental health (64.94 [self-employed] vs 59.23 [housewives], P = 0.007). They also suffered from less bodily pain (P = 0.042). Frequency of dialysis resulted in significant changes in general health (P < 0.001), vitality (P = 0.011), social functioning (P = 0.017), and mental health (P = 0.009), and three sessions of dialysis per day resulted in better general health (55.58), vitality (55.5), social functioning (75), and mental health (68.26). Having a separate room for dialysis also had a significant association with better scores of general health (50 [self-employed] vs 40 [housewives], P = 0.023), social functioning (75 [self-employed] vs 62 [housewives], P = 0.015), VT (55 [self-employed] vs 45 [housewives], P = 0.048), RE (66 [self-employed] vs 0 [housewives], P = 0.002), and MH (68 [self-employed] vs 54 [housewives], P = 0.014). No relation was observed between patients level of Hb and quality of life; however, higher levels of Hb in patients were associated with a better role physical (P = 0.007).
Although the duration of dialysis did not demonstrate significant association with any of the QoL sub-scales, dialysis adequacy established a significant association with vitality (P = 0.06) and social functioning (P = 0.029), where higher dialysis adequacy provided better outcomes. Duration of disease was also associated with physical functioning (P = 0.017), and patients with a shorter duration of kidney disease had a better physical functioning. In addition, residual renal function was significantly associated with better role physical (P = 0.24) and mental health (P = 0.035) (see Table 4).
Table 4: Association of each contributing factor with SF-36 QoL questionnaire sub-scales.
| SF-36 subscales | Gendera | Marriagea | Dialysis frequencyb | Seperate room for dialysisa | Employmentb | Agec | BMIc | Duration of dialysis | Residual renal function | Dialysis adequacy | Hemoglobin (g/dL)c | Disease durationc | Comorbiditiese |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PF | 0.010* | 0.217 | 0.235 | 0.798 | 0.003* | <0.001* | 0.811 | 0.902 | 0.020* | 0.535 | 0.148 | 0.017* | 0.394 |
| RP | <0.001* | 0.328 | 0.732 | 0.051 | <0.001* | 0.923 | 0.740 | 0.663 | 0.024* | 0.334 | 0.007* | 0.621 | 0.403 |
| BP | 0.033* | 0.278 | 0.681 | 0.40 | 0.042* | 0.171 | 0.425 | 0.352 | 0.093 | 0.166 | 0.099 | 0.511 | 0.334 |
| GH | 0.049* | 0.112 | <0.001* | 0.023* | 0.014* | 0.315 | 0.946 | 0.911 | 0.108 | 0.827 | 0.250 | 0.111 | 0.468 |
| VT | 0.163 | 0.520 | 0.011* | 0.048* | 0.169 | 0.763 | 0.544 | 0.868 | 0.075 | 0.06* | 0.606 | 0.304 | 0.377 |
| SF | 0.788 | 0.260 | 0.017* | 0.015* | 0.860 | 0.882 | 0.236 | 0.774 | 0.177 | 0.029* | 0.494 | 0.393 | 0.477 |
| RE | 0.016* | 0.888 | 0.065 | 0.002* | 0.007* | 0.236 | 0.705 | 0.863 | 0.201 | 0.211 | 0.126 | 0.490 | 0.769 |
| MH | 0.122 | 0.111 | 0.009* | 0.014* | 0.007* | 0.064 | 0.372 | 0.448 | 0.035* | 0.469 | 0.381 | 0.586 | 0.670 |
PF: physical functioning, RP: role limitations due to physical health, BP: bodily pain, GH: general health, VT: energy/fatigue vitality, SF: social functioning, RE: role limitations due to emotional problems, MH: mental health, emotional well-being. *The test is significant at P = 0.05.
The mean sub-scale scores across contributing factors are presented in Table A1.
Discussion
This study discovered that the most significant characteristics independently associated with quality of life were gender, employment, frequency of dialysis, and residual renal function. In the present study, males had a higher total QoL score than females (58.18 in males, compared to 48.18 in females). On the other hand, in subgroup analysis, males had a better score for physical functioning than females (70 in males, compared to 55 in females). Similar to our findings, studies in North America showed males to be associated with better quality of life (32, 33). In addition, some European studies using the SF-36 discovered an association between males and better QoL (34, 35). In contrast, other studies conducted in the United Kingdom and Turkey determined that scores for males were independently associated with a lower score for all QoL dimensions (9, 24). Previous studies demonstrated that faster decline in kidney function in males than in females could have a negative impact on HRQoL in males, while changes in the hypothalamic–pituitary–gonadal hormones status could make females more prone to problems such as sleep disorders, depression, and cognitive dysfunction (36, 37). On the other hand, males socialized in a different manner than females, more independent and self-controlled, especially in Middle East cultures, while females are taught to be more emotionally expressive, dependent, and concerned with their physical appearance to be accepted by the society (38). It seems that gender roles are not rigid or fixed and depend on some qualitative issues, such as ethnicity, culture, family dynamics, coping mechanisms, educational and social factors as well as physiologic hormonal status. Further studies are required to explore gender roles on quality of life in PD patients. In the present study, notwithstanding the previous studies (34, 39), married patients had no significantly better quality of life, indicating that most patients, either single or married, experienced good support through family ties, maybe due to traditional Iranian culture. According to results of the present study, frequency of dialysis was significantly associated with quality of life. It was not surprising to observe the negative effects of frequency of dialysis on the quality of life of patients because of the time required to spend on dialysis. Self-employed patients were significantly associated with a higher QoL score in our population. It was documented that employment not only provided economic benefits but increased self-esteem, sense of control, and social value (24, 40). On the other hand, the Brazilian peritoneal dialysis multi-center study demonstrated that quality of life was not significantly associated with family income (41), while other aspects of working beyond financial matters might influence more the quality of life. In the present study, patients who were self-employed and could schedule their working time themselves, experienced better quality of life than those working for others. Another factor that was not associated with QoL score in our population was education. However, poor educational status was shown to have a negative effect on the quality of life of PD patients in other studies (24, 33–35). The most common comorbidity in patients of the present study was diabetes mellitus. In the present study, comorbidities were not associated with any sub-scale of quality of life, while another study showed that diabetic patients scored significantly worse on the physical function scale. Although in certain surveys, some comorbidities were related to some QoL sub-scale scores, other possible reasons could be observed for lacking a significant association between the QoL sub-scale scores and diseased condition (24, 34). It appeared that quality of life was not determined merely by the absence or presence of comorbidities; however, it was influenced by patients’ perception of their position in different aspects of life, and many non-disease health-related factors play important roles (42). Besides, the severity of comorbidities should be considered in the future studies. Our study demonstrated no significant association between age and QoL score. However, a Spanish study showed that advanced age adversely affects the QoL score (34). It is important to note that in the present study, a significant association between mental health sub-scale and residual renal function was established. This result was consistent with the results of previous studies, indicating that higher residual renal function was associated with improved HRQoL of PD patients, particularly in mental health domains (43, 44). Dialysis adequacy was significantly associated with social functioning and vitality sub-scales. Scarce data were available regarding the effect of dialysis adequacy on the physical and mental domains of quality of life (45, 46), whereas other studies showed no significant association (24, 47).
In contrast with other studies, no statistically significant relationship was observed in the present study between Hb level and the QoL score in peritoneal dialysis patients (2, 48, 49). However, higher Hb levels were associated with a better score of role physical sub-scale (P = 0.007). This result was consistent with another study, where greater Hb concentration was related to better QoL scores on physical dimension (35).
Strength and limitations of the study
We conducted a multi-center study and applied the SF-36 questionnaire that has been widely used in various studies so that the results could reflect local conditions. No information was collected on the psychological features of the patients, structure of services, patients’ satisfaction with healthcare services, and healthcare profession–patient relationship. The future studies should consider these aspects for a comprehensive view of the quality of life of PD patients.
Conclusion
Our study showed that the most significant characteristics that were independently associated with patient’s quality of life were gender, employment, residual renal function, and frequency of dialysis. Evaluation of quality of life should be incorporated in clinical follow-up of PD patients The above-mentioned factors should be considered to a greater extent for implementing strategies and possible interventions to improve certain aspects of quality of life in our population.
Acknowledgments
This study was supported by Isfahan University of Medical Sciences (Project No.: 398599).
Conflict of interest
The authors declared no potential conflicts of interest with respect to research, authorship and/or publication of this article.
Availability of data and materials
The datasets during and/or analyzed during the current study available from the corresponding author on reasonable request.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author contributions
Niloofar Nili and Mojgan Mortazavi researched literature and conceived the study. SM Hosseini and M Kazemi Naeini did data analysis. Niloofar Nili and Mojgan Mortazavi wrote the first draft of the manuscript, and the latter revised the article. All authors were involved in protocol development. Finally, all authors reviewed and edited, and approved the final version of the manuscript.
REFERENCES
1. Eggers PW. Has the incidence of end-stage renal disease in the USA and other countries stabilized? Curr Opin Nephrol Hypertens. 2011 May 1;20(3):241–5. 10.1097/MNH.0b013e3283454319
2. Okpechi IG, Nthite T, Swanepoel CR. Health-related quality of life in patients on hemodialysis and peritoneal dialysis. Saudi J Kidney Dis Transplant. 2013 May 1;24(3):519. 10.4103/1319-2442.111036
3. Afshar R, Sanavi S, Salimi J. Epidemiology of chronic renal failure in Iran: A four-year single-center experience. Saudi J Kidney Dis Transplant. 2007 Apr 1;18(2):191.
4. Morovatdar N, Tayebi Nasrabad G, Tsarouhas K, Rezaee R. Etiology of renal replacement therapy in Iran. Int J Nephrol. 2019 Nov 26;2019. 10.1155/2019/5010293
5. Beladi MS, Sametzadeh M, Hayati F, Fatemi SM. Evaluation of acquired cystic kidney disease in patients on hemodialysis with ultrasonography. Iran J Kidney Dis. 2010 Jul;4(3):223–6
6. Aghighi M, Mahdavi MM, Zamyadi M, Heydari RA, Rajolani H, Nourouzi S. Changing epidemiology of end-stage renal disease in last 10 years in Iran. Iran J Kidney Dis. 2009 Oct;3(4):192–6
7. Malekmakan L, Haghpanah S, Pakfetrat M, Malekmakan A, Khajehdehi P. Causes of chronic renal failure among Iranian hemodialysis patients. Saudi J Kidney Dis Transplant. 2009 May 1;20(3):501.
8. Mousavi SS, Hayati F, Mousavi M. What is the difference between causes of ESRD in Iran and developing countries?. Shiraz E-Med J. 2012;13(2):e93952.
9. Sayin A, Mutluay RÜ, Sindel S. Quality of life in hemodialysis, peritoneal dialysis, and transplantation patients. Transplant Proc. 2007 Dec 1;39(10):3047–3053. Elsevier. 10.1016/j.transproceed.2007.09.030
10. Subha Palaneeswari M, Rajan PA, Silambanan Santhi J. Blood lead in end-stage renal disease (ESRD) patients who were on maintainence haemodialysis. J Clin Diagn Res (JCDR). 2012 Dec;6(10):1633. 10.7860/JCDR/2012/4865.2627
11. Braunwald F, Kasper H, Longo J. Disturbances of the renal function. In: Harrison’s principles of intenal medicine, vol. 2. 15th ed. McGraw Hill; 2004, pp. 1535–41.
12. Port FK, Wolfe RA, Mauger EA, Berling DP, Jiang K. Comparison of survival probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA. 1993 Sep 15;270(11):1339–43. 10.1001/jama.270.11.1339
13. Jain D, Haddad DB, Goel N. Choice of dialysis modality prior to kidney transplantation: Does it matter? World J Nephrol. 2019 Jan 21;8(1):1. 10.5527/wjn.v8.i1.0000
14. Noshad H, Sadreddini S, Nezami N, Salekzamani Y, Ardalan MR. Comparison of outcome and quality of life: Haemodialysis versus peritoneal dialysis patients. Singapore Med J. 2009 Feb 1;50(2):185.
15. Mahdavi-Mazdeh M, Zamyadi M, Nafar M. Assessment of management and treatment responses in haemodialysis patients from Tehran province, Iran. Nephrol Dial Transplant. 2008 Jan 1;23(1):288–93. 10.1093/ndt/gfm580
16. Chuasuwan A, Pooripussarakul S, Thakkinstian A, Ingsathit A, Pattanaprateep O. Comparisons of quality of life between patients underwent peritoneal dialysis and hemodialysis: A systematic review and meta-analysis. Health Qual Life Outcomes. 2020 Dec;18(1):1. 10.1186/s12955-020-01449-2
17. Zee J, Zhao J, Subramanian L, Perry E, Bryant N, McCall M, et al. Perceptions about the dialysis modality decision process among peritoneal dialysis and in-center hemodialysis patients. BMC Nephrol. 2018 Dec;19(1). 10.1186/s12882-018-1096-x
18. Morton RL, Snelling P, Webster AC, Rose J, Masterson R, Johnson DW, Howard K. Factors influencing patient choice of dialysis versus conservative care to treat end-stage kidney disease. CMAJ. 2012 Mar 20;184(5):E277–83. 10.1503/cmaj.111355
19. He Z, Hou H, Zhang D, Mo Y, Zhang L, Su G, et al. Effects of dialysis modality choice on the survival of end-stage renal disease patients in southern China: A retrospective cohort study. BMC Nephrol. 2020 Dec;21(1):1–1. 10.1186/s12882-020-02070-7
20. World Health Organization (WHO). Programme on mental health: WHO QOL user manual. World Health Organization; 1998.
21. Ramos EC, Santos ID, Zanini RD, Ramos JM. Quality of life of chronic renal patients in peritoneal dialysis and hemodialysis. Braz J Nephrol. 2015 Sep;37(3):297–305. 10.5935/0101-2800.20150049
22. Haghighi M, Heydari RA, Zamyadi M, Mahdavi MM, Nourouzi S, Rajolani H, et al. Dialysis in Iran. Iran. Red. Crescent. Med. J. [Internet]. 2020 Sep. 30 [cited 2023 Feb. 25];22(9). Available from: https://www.ircmj.com/index.php/IRCMJ/article/view/143
23. Eser E, Fidaner H, Eser SY, Fidaner C, Elbi H. Derivation of response scales for WHO QOL TR: The effect of the level of education on the use of Visual Analog Scales. Eur Psychol. 2000 Dec;5(4):278. 10.1027//1016-9040.5.4.278
24. Bakewell AB, Higgins RM, Edmunds ME. Quality of life in peritoneal dialysis patients: Decline over time and association with clinical outcomes. Kidney Int. 2002 Jan 1;61(1):239–48. 10.1046/j.1523-1755.2002.00096.x
25. Pezeshki M, Rostami Z. Contributing factors in health-related quality of life assessment of ESRD patients: A single center study. Nephro Urol Mon. 2009 Dec 31;1(2):129–36.
26. Zazzeroni L, Pasquinelli G, Nanni E, Cremonini V, Rubbi I. Comparison of quality of life in patients undergoing hemodialysis and peritoneal dialysis: A systematic review and meta-analysis. Kidney Blood Press Res. 2017;42(4):717–27. 10.1159/000484115
27. Jofre R, López-Gómez JM, Valderrábano F. Quality of life for patient groups. Kidney Int. 2000 Jan 1;57:S121–30. 10.1046/j.1523-1755.2000.07420.x
28. Lew SQ, Piraino B. Quality of life and psychological issues in peritoneal dialysis patients. Semin Dial. 2005 Mar 4;18(2):119–23. Blackwell Science Inc., Oxford, UK. 10.1111/j.1525-139X.2005.18215.x
29. Al Wakeel J, Al Harbi A, Bayoumi M, Al-Suwaida K, Al Ghonaim M, Mishkiry A. Quality of life in hemodialysis and peritoneal dialysis patients in Saudi Arabia. Ann Saudi Med. 2012 Nov;32(6):570–4. 10.5144/0256-4947.2012.570
30. Daugirdas JT, Blake PG, Ing TS. Handbook of dialysis. Philadelphia, PA: Lippincott Williams & Wilkins; 2012.
31. Montazeri A, Gashtasbi A, Vahdaninya M. Translate and determine the validity and reliability of such questionnaires Persian SF36. Payesh J. 2005;5(1):49–56.
32. Sehgal AR. Outcomes of renal replacement therapy among blacks and women. Am J Kidney Dis. 2000 Apr 1;35(4):S148–52. 10.1016/S0272-6386(00)70242-3
33. Rocco MV, Gassman JJ, Wang SR, Kaplan RM. Cross-sectional study of quality of life and symptoms in chronic renal disease patients: The modification of diet in renal disease study. Am J Kidney Dis. 1997 Jun 1;29(6):888–96. 10.1016/S0272-6386(97)90463-7
34. Mingardi, G., Cornalba, L., Cortinovis, E., Ruggiata, R., Mosconi, P., Apolone, G.. Health-related quality of life in dialysis patients. A report from an Italian study using the SF-36 Health Survey. DIA-QOL Group. Nephrol Dial Transplant. 1999;14(6):1503–10. (Official Publication of the European Dialysis and Transplant Association-European Renal Association.) 10.1093/ndt/14.6.1503
35. Moreno, F., Gomez, JL., Sanz-Guajardo, D., Jofre, R., Valderrabano, F., Spanish Cooperative Renal Patients Quality of Life Study Group 4. Quality of life in dialysis patients. A Spanish multicentre study. Nephrol Dial Transplant. 1996 Jan 1;11(Supp2):125–9. 10.1093/ndt/11.supp2.125
36. Weisinger JR, Bellorin-Font E. Outcomes associated with hypogonadism in women with chronic kidney disease. Adv Chronic Kidney Dis. 2004 Oct 1;11(4):361–70. 10.1053/j.ackd.2004.07.009
37. Aguiar R, Pei M, Qureshi AR, Lindholm B. Health-related quality of life in peritoneal dialysis patients: A narrative review. Semin Dial. 2019 Sep;32(5):452–62. 10.1111/sdi.12770
38. Ogutmen B, Yildirim A, Sever MS, Bozfakioglu S, Ataman R, Erek E, et al. Health-related quality of life after kidney transplantation in comparison intermittent hemodialysis, peritoneal dialysis, and normal controls. Transplant Proc. 2006 Mar 1;38(2):419–421. Elsevier. 10.1016/j.transproceed.2006.01.016
39. Overbeck I, Bartels M, Decker O, Harms J, Hauss J, Fangmann J. Changes in quality of life after renal transplantation. Transplant Proc. 2005 Apr 1;37(3):1618–21. Elsevier. 10.1016/j.transproceed.2004.09.019
40. Plantinga LC, Fink NE, Harrington-Levey R, Finkelstein FO, Hebah N, Powe NR, et al. Association of social support with outcomes in incident dialysis patients. Clin J Am Soc Nephrol. 2010 Aug 1;5(8):1480–8. 10.2215/CJN.01240210
41. dos Santos Grincenkov FR, Fernandes N, dos Santos Pereira B, Bastos K, Lopes AA, Finkelstein FO, et al. Impact of baseline health-related quality of life scores on survival of incident patients on peritoneal dialysis: A cohort study. Nephron. 2015;129(2):97–103. 10.1159/000369139
42. Rebollo P, Ortega F, Baltar JM, Badía X, Alvarez-Ude F, Díaz-Corte C, et al. Health-related quality of life (HRQOL) of kidney transplanted patients: Variables that influence it. Clin Transplant. 2000 Jun;14(3):199–207. 10.1034/j.1399-0012.2000.140304.x
43. Park HC, Lee H, Lee JP, Kim DK, Oh KH, Joo KW, et al. Lower residual renal function is a risk factor for depression and impaired health-related quality of life in Korean peritoneal dialysis patients. J Korean Med Sci. 2012 Jan;27(1):64. 10.3346/jkms.2012.27.1.64
44. Shafi T, Jaar BG, Plantinga LC, Fink NE, Sadler JH, Parekh RS, et al. Association of residual urine output with mortality, quality of life, and inflammation in incident hemodialysis patients: The Choices for Healthy Outcomes in Caring for End-Stage Renal Disease (CHOICE) Study. Am J Kidney Dis. 2010;56(2):348–58. 10.1053/j.ajkd.2010.03.020
45. Sunder S, Kalra OP, Nashine S, Waghmare V, Ruchi R. Comparative study of adequacy of dialysis and health-related quality of life in patients on CAPD and APD. Perit Dial Int. 2008 Sep;28(5):542–4. 10.1177/089686080802800521
46. Chen YC, Hung KY, Kao TW, Tsai TJ, Chen WY. Relationship between dialysis adequacy and quality of life in long-term peritoneal dialysis patients. Perit Dial Int. 2000 Sep;20(5):534–40. 10.1177/089686080002000508
47. Paniagua R, Amato D, Vonesh E, Guo A, Mujais S. Health-related quality of life predicts outcomes but is not affected by peritoneal clearance: The ADEMEX trial. Kidney Int. 2005 Mar 1;67(3):1093–104. 10.1111/j.1523-1755.2005.00175.x
48. Okaka EI, Davies M, Ahmed M, Naidoo S, Naicker S. Impact of socio-economic factors on quality of life in patients on continuous ambulatory peritoneal dialysis in an African setting. W Afr J Med. 2014 Apr 1;33(2):125–9.
49. Maor Y, King M, Olmer L, Mozes B. A comparison of three measures: The time trade-off technique, global health-related quality of life and the SF-36 in dialysis patients. J Clin Epidemiol. 2001 Jun 1;54(6):565–70. 10.1016/S0895-4356(00)00338-3
Appendix
Table A1: Mean (SD) values of each contributing factor regarding each of SF-36 QoL questionnaire sub-scales.
| Subscales of questionnaire | PF | RP | BP | GH | VT | SF | RE | MH | |
|---|---|---|---|---|---|---|---|---|---|
| Gender | Male | 70 (35) | 50 (75) | 87.5 (36.88) | 50 (25) | 50 (30) | 62.5 (25) | 66.66 (100) | 68 (31) |
| Female | 55 (65) | 0 (50) | 77.5 (55) | 40 (35) | 50 (30) | 62.5 (50) | 0 (100) | 60 (44) | |
| Having separate room | Yes | 70 (50) | 25 (75) | 80 (55) | 50 (35) | 55 (35) | 75 (35.5) | 66.66 (100) | 68 (32) |
| No | 65 (40) | 0 (50) | 77.5 (45) | 40 (22.5) | 45 (20) | 62.5 (25) | 0 (100) | 54 (34) | |
| Employment | Housewife | 49.71 (31.64) | 0 (100) | 77.5 (52.5) | 44.23 (19.63) | 48.65 (19.73) | 67.06 (23.48) | 0 (58.33) | 59.23 (22.60) |
| Retired | 59 (22.46) | 62.5 (100) | 77.5 (47.5) | 48.83 (19.83) | 54.66 (19.38) | 66.66 (21.60) | 100 (100) | 70.66 (17.61) | |
| Employed | 69.09 (22.13) | 75 (75) | 90 (35) | 54.18 (16.46) | 52.63 (18.45) | 69.09 (20.95) | 66.66 (100) | 64.94 (22.37) | |
| Dialysis frequency | 1 or 2 | 70 (48.75) | 0 (75) | 95 (35) | 51.66 (19.22) | 55.41 (17.11) | 75 (46.88) | 0 (100) | 66.66 (24.73) |
| 3 | 75 (43.75) | 23 (75) | 77.5 (45) | 55.58 (17.70) | 55.5 (17.36) | 75 (37.5) | 50 (100) | 68.26 (19.66) | |
| 4 | 55 (45) | 0 (75) | 77.5 (45) | 44.95 (19.42) | 47.98 (21.02) | 62.5 (25) | 0 (100) | 59.87 (23.58) | |
| 5 or 6 | 60 (23.75) | 12.5 (50) | 77.5 (15) | 34.37 (11.52) | 39.37 (17.11) | 50 (12.5) | 0 (50) | 50.25 (18.64) | |
PF: physical functioning, RP: role limitations due to physical health, BP: bodily pain, GH: general health, VT: energy/fatigue vitality, SF: social functioning, RE: role limitations due to emotional problems, MH: mental health, emotional well-being. Median (interquartile range) was reported for non-normal variables, and mean (SD) was reported for normal variables.