
Download
CASE REPORT: HEPATOLOGY
Acute Hepatitis by Bartonella henselae Infection in an Adult Patient with Decompensated Liver Cirrhosis
Jorge Alonso Garay-Ortega1*, Louis Fernando Robles Fernandes2, Vianey Guadalupe Téllez Bolaños2, Karla Paulina Sandoval Mosqueda1, Karla Daniela Salgado Guizar2
1Resident Physician in Gastroenterology, National Medical Center Siglo XXI of the Mexican Social Security Institute, Mexico City, Mexico;
2Resident Physician in Internal Medicine, National Medical Center Siglo XXI of the Mexican Social Security Institute, Mexico City, Mexico
Abstract
Hepatitis caused by Bartonella henselae in adults is a condition that is seldom reported in the literature, as well as its current incidence and prevalence. While there is a broad spectrum of well-defined and established clinical entities, hepatic involvement represents the third most frequent clinical manifestation of infection by this genus of bacteria. It may or may not be characterized by the presence of hepatosplenic granulomas. Diagnosis requires a high level of clinical suspicion, exclusion of additional etiologies, and a causal relationship with risk factors. Polymerase chain reaction is the diagnostic test with the highest diagnostic yield, and treatment varies depending on the clinical expression. We describe the case of an adult patient with hepatitis secondary to Bartonella henselae infection.
Key words: adult, Bartonella, gastroenterology, hepatitis, hepatology
Author for correspondence: Jorge Alonso Garay-Ortega, Resident Physician in Gastroenterology, National Medical Center Siglo XXI of the Mexican Social Security Institute, Mexico City, Mexico. Email: jorge.garay11@hotmail.com
Received: 4 August 2023; Accepted after Revision: 17 August 2023; Published: 30 August 2023
DOI: 10.15586/jrenhep.v7i2.172
Copyright: Garay-Ortega JA, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
The genus Bartonella spp. belongs to a group of gram-negative, aerobic, non-motile bacteria that behave as facultative intracellular pathogens. It can cause a range of zoonotic diseases and can be considered as both emerging and re-emerging pathogens1. Various clinical entities result from infection with this group of bacteria, with notable examples including cat-scratch disease, bacillary angiomatosis, trench fever, and Carrion’s disease, among other manifestations. Worth mentioning is hepatic involvement with or without the formation of hepatosplenic granulomas1. The main species of Bartonella implicated in human diseases are B. henselae and B. quintana. These can be transmitted by vectors such as cats and utilize mammals as reservoirs. They infect similar types of cells (endothelial cells and erythrocytes) and induce vasculoproliferative changes in immunocompromised patients; they can also affect immunocompetent individuals1.
At present, exact and precise figures for the incidence and prevalence of the disease are lacking; only estimates are available, which may not accurately represent the current disease situation. A study conducted in the United States showed an approximate incidence of 6.4 cases per 100,000 inhabitants, and it is estimated that there is one cat for every 5.4 inhabitants in a given region2. In Mexico, there are limited figures on this disease due to few reports. There has been a single case series reported by the pediatric infectious disease service at the former Civil Hospital of Guadalajara, along with sporadic reports of isolated cases, mostly involving children with prolonged febrile syndrome and adenopathy3. At the time of writing this article, there have been no published reports of Bartonella spp. infection in adults in Mexico. This case report is that of a male patient with acute hepatitis secondary to confirmed Bartonella spp. infection, following extensive clinical and biochemical evaluation, and also liver cirrhosis associated with fatty liver disease.
Case Report
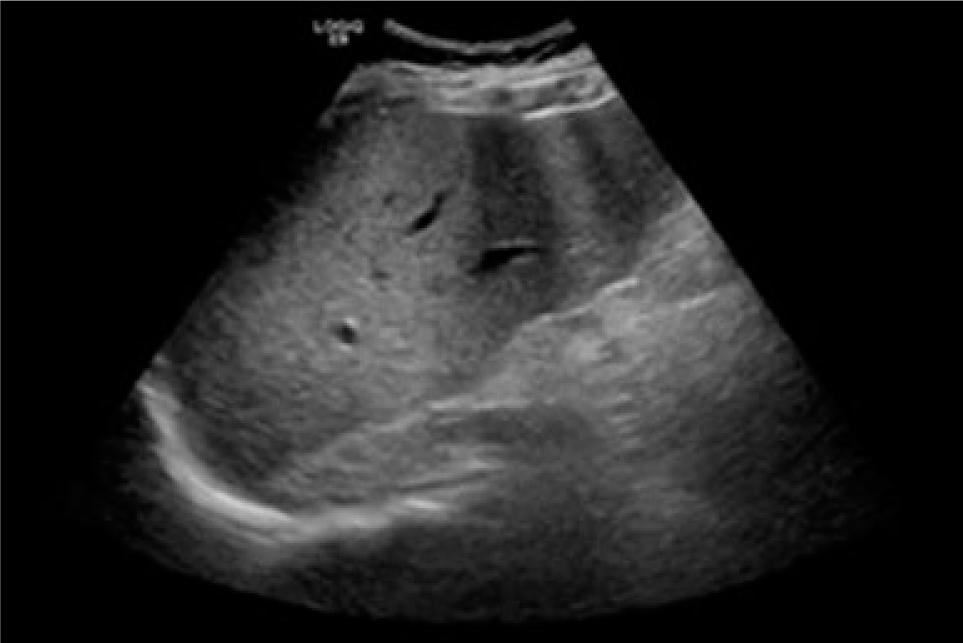
A 28-year-old man with no relevant family history presented with a history of living with multiple cats at home. He was diagnosed with a craniopharyngioma at the age of 15, underwent partial tumor resection in the same year; he also was diagnosed with type 2 diabetes at the age of 28, and experienced pulmonary thromboembolism at the age of 19 following a car accident with pelvic trauma. His body mass index was 34.6 kg/m2. During an endocrinology follow-up, the following laboratory results were reported: total bilirubin 3.15 mg/dL, direct bilirubin 1.22 mg/dL, indirect bilirubin 1.93 mg/dL, AST 60 U/L, ALT 41 U/L, gamma-glutamyl transferase (GGT) 84 U/L, alkaline phosphatase 146 U/L, hemoglobin 15.1 g/dL, and platelets 38,000 cells/mm3. Given a suspicion of hepatopathy, viral panel testing for hepatitis B virus, hepatitis C virus, and human immunodeficiency virus returned negative results. Autoimmune causes were also ruled out through serological tests. An abdominal ultrasound revealed grade 2 hepatic steatosis, splenomegaly, intrahepatic biliary duct dilation, and elastography indicating fibrosis (Figure 1). Ultrasound-guided biopsy showed characteristic changes of hepatic cirrhosis. The underlying cause of the hepatopathy was determined to be metabolism-associated fatty liver disease.
Figure 1: Abdominal ultrasound with findings consistent with chronic hepatopathy.
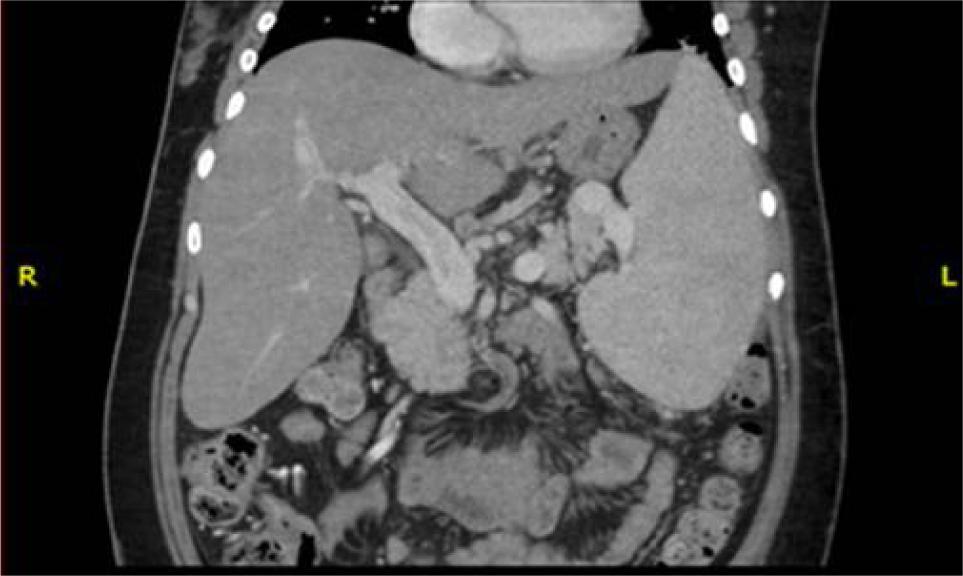
A month later, the patient presented to our medical unit with coffee ground vomiting and a recent episode of melena. His vital signs included blood pressure of 90/50 mmHg, heart rate of 92 beats per minute, respiratory rate of 20 breaths per minute, and temperature of 38.5°C. Physical examination revealed abdominal tenderness upon deep palpation of the epigastrium. Laboratory studies showed glucose 69 mg/dL, sodium 146 mEq/L, chloride 112 mEq/L, hemoglobin 9.6 g/dL, platelets 33,000 cells/mm3, neutrophils 3700 cells/mm3, total bilirubin 1.26 mg/dL, direct bilirubin 0.53 mg/dL, indirect bilirubin 0.73 mg/dL, AST 18 U/L, ALT 18 U/L, LDH 146 U/L, and C-reactive protein at 11 mg/dL. An upper endoscopy revealed large esophageal varices (Baveno VII) with signs of recent bleeding, for which it was necessary to perform variceal ligation and use terlipressin. The patient developed fever during hospitalization, and a chest X-ray indicated an alveolar pattern suggestive of infection. Antibiotic therapy with piperacillin-tazobactam was initiated, followed by meropenem and vancomycin due to the lack of improvement. The patient’s condition deteriorated further, with worsening general status, dyspnea at rest, heart rate exceeding 110 beats per minute, and right hypochondrial abdominal pain associated with hepatomegaly. Abdominal angiotomography revealed mesenteric vein ectasia, chronic thrombosis of some branches, portal hypertension, hepatic steatosis, and hepatosplenomegaly (Figure 2).
Figure 2: Abdominal angiotomography in coronal plane highlighting splenomegaly and hepatomegaly despite the diagnosis of cirrhosis.
Testing for adenosine deaminase and nucleic acid amplification for tuberculosis yielded negative results. A whole-body scan and single-photon emission computed tomography (SPECT) abdomen scan showed no evidence of infectious or inflammatory processes. Despite successful control of variceal bleeding, the patient continued to experience anemia and later developed pancytopenia (hemoglobin 7.5 g/dL, platelets 27,000 cells/mm3, neutrophils 1000 cells/mm3). Liver function tests remained stable throughout the clinical course: albumin 2.9 g/dL, total bilirubin 0.95 mg/L, AST 60 U/L, ALT 92 U/L, alkaline phosphatase 75 U/L, and GGT 75 U/L. Due to a history of cat exposure, Bartonella henselae hepatitis was suspected, and polymerase chain reaction (PCR) testing returned a positive result. The patient was initiated on intravenous rifampicin 300 mg every 12 h and oral azithromycin 500 mg on the first day, followed by 250 mg daily for a total of 10 days. After completing the treatment regimen, fever episodes subsided and biochemical parameters improved (hemoglobin 8.6 g/dL, platelets 145,000 cells/mm3, neutrophils 5200 cells/mm3, total bilirubin 0.26 mg/dL, ALT 13 U/L, AST 29 U/L, alkaline phosphatase 117 U/L, GGT 98 U/L, C-reactive protein 2 mg/dL). The patient continued to be monitored at our unit, but unfortunately, he succumbed to complications associated with decompensated liver cirrhosis months later.
Discussion
Bartonella spp. infection in adults poses a diagnostic challenge and requires a high level of clinical suspicion, as well as exclusion of more common etiologies. The most common presentation in immunocompetent hosts is self-limiting fever and regional lymphadenopathy. Immunocompromised hosts can develop pathological vasoproliferation associated with abundant collections of organisms, such as bacillary peliosis (found in 71.4% of cases) involving the liver and spleen, or bacillary angiomatosis, which can be cutaneous or visceral. The balance between granulomatous and vasoproliferative manifestations is believed to be host-dependent4.
Hepatic involvement in bartonellosis is reported in approximately 1–2% of cases and represents the third most frequent presentation of the disease after fever and lymphadenopathy. Typical clinical manifestations include nonspecific symptoms like right upper quadrant pain, headache, chills, fever, weight loss, and malaise5. In our patient, the symptoms corresponded to those described, with only slight increases in liver enzyme levels, characterized by mild elevation of aminotransferases and GGT. Notably, pancitopenia was observed and improved following initiation of Bartonella antimicrobial therapy.
Diagnosis requires three of the following elements: (1) history of animal contact, (2) scratch or primary dermal or ocular lesion, (3) regional lymphadenopathy, (4) positive serology (greater than 1:256), or (5) positive lymph node biopsy6. Imaging evaluation is typically performed through simple or contrast-enhanced tomography, which may reveal lesions of heterogeneous density including hypodense, isodense, or ring-enhancing patterns. Magnetic resonance imaging findings can also elucidate the presence of granulomas5. Histopathological analysis reveals necrotizing granulomas with macrophage accumulation surrounded by fibroblast infiltration and lymphocytes5, which are not specific to the disease.
Currently, PCR testing provides the best diagnostic performance, although serological analysis against Bartonella spp. antigens, specific immunohistochemical staining, or even silver staining of Steiner are alternative options, albeit with lower sensitivity5. In our patient, the history of cat exposure, occasional scratches by cats, and positive PCR testing contributed to the Bartonella diagnosis.
For hepatosplenic involvement associated with fever of unknown origin, first-line treatment typically involves a macrolide combined with rifampicin for a period of 10–14 days, with or without the addition of corticosteroids for severe or persistent disease7. In our case, the patient reported symptom improvement, and biochemical parameters improved after completion of treatment, without the need for corticosteroid use, leading to his discharge.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Informed consent was obtained from the patient authorizing the development of this case report.
Footnotes
How to cite: Garay-Ortega JA, et al. Acute Hepatitis by Bartonella henselae Infection in an Adult Patient with Decompensated Liver Cirrhosis. J Ren Hepat Disord. 2023;7(2): 15–17.
REFERENCES
1. Ramón Blanco J, Raoult D. Enfermedades producidas por Bartonella spp. Diseases produced by Bartonella. Enferm Infecc Microbiol Clín. 2005;23(5):313–20. 10.1157/13074971
2. Nelson CA, Moore AR, Perea AE, Mead PS. Cat scratch disease: U.S. clinicians’ experience and knowledge. Zoonoses Public Health. 2018;65(1):67–73. 10.1111/zph.12368
3. Guerrero-Becerra M, de León-Herrera SR, Plascencia-Hernández A, Mercado-Uribe MC, Martínez-Arce P, Luévanos-Velázquez A, et al. Enfermedad por arañazo de gato (EAG), experiencia del Hospital Civil de Guadalajara (HCG), México. Bol Clin Hosp Infant Edo Son. 2018;35(1):61–9.
4. Rostad CA, McElroy AK, Hilinski JA, Thompson MP, Drew CP, Denison AM, et al. Bartonella henselae-mediated disease in solid organ transplant recipients: Two pediatric cases and a literature review. Transpl Infect Dis. 2012;14(5):E71–81. 10.1111/j.1399-3062.2012.00774.x
5. VanderHeyden TR, Yong SL, Breitschwerdt EB, Maggi RG, Mihalik AR, Parada JP, et al. Granulomatous hepatitis due to Bartonella henselae infection in an immunocompetent patient. BMC Infect Dis. 2012;12:17. 10.1186/1471-2334-12-17
6. Opavsky MA. Cat scratch disease: The story continues. Can J Infect Dis. 1997;8(1):43–9. 10.1155/1997/982908
7. Prutsky G, Domecq JP, Mori L, Bebko S, Matzumura M, Sabouni A, et al. Treatment outcomes of human bartonellosis: A systematic review and meta-analysis. Int J Infect Dis. 2013;17(10):e811–19. 10.1016/j.ijid.2013.02.016