
Download
ORIGINAL ARTICLE: NEPHROLOGY
Prevalence of dysmagnesemia among CKD patients in North India
Shailata Prisi1, Kajal Nandi1, Elvia Jamatia2*, Biplob Kumar Biswas3, Vatsala Khurana4, Binita Goswami1
1Department of Biochemistry, Maulana Azad Medical College, New Delhi, India;
2Department of Biochemistry, Dr. Baba Saheb Ambedkar Medical College, Rohini, New Delhi, India;
3Department of Laboratory Medicine, Jaypee Hospital, Noida, UP, India;
4Department of Genomic Medicine, Queen Mary University of London, UK
Abstract
Magnesium is the second-most common intracellular cation after calcium with 99% of total body magnesium distributed intracellularly in bones, muscles, and soft tissues. Only 1% of total body magnesium is present extracellularly that contributes to the normal serum magnesium concentration of 1.8–2.6 mg/dL. Recently, many studies have focused on the role of magnesium homeostasis and human health. Diabetes and hypertension are the leading causes of chronic kidney disease (CKD), and the significance of magnesium in CKD has been astonishing in medical practice. In this study, we investigated the serum levels of magnesium and its prevalence at different stages of CKD. This cross-sectional descriptive study was conducted over a period of 2 months. Serum magnesium levels were analysed in 224 patients with CKD and were grouped into five stages of CKD according to the guidelines of the Kidney Disease: Improving Global Outcomes (KDIGO) based on glomerular filtration rate. Laboratory data of patients was analysed using the IBM SPSS V23 software (Chicago, USA) for statistical relationship between serum magnesium levels and stages of CKD in patients with CKD. Mean serum magnesium level of the study population was 2.21 ± 0.75 mg/dL; 50.9% of the patients were normomagnesemic (normal level of magnesium ions in the blood), followed by 30.4% hypomagnesemic and 20.5%, hypermagnesemic. CKD was more common in males (63.4%), compared to females (36.6%). Mean age of patients in G5 stage was significantly higher than in G3a, G3b, and G4 stages (P = 0.001). A progressive decline in renal function and retention of uraemic solutes was observed with progression of CKD. Multiple factors, both inherited or acquired, such as diuretics and alcohol, are implicated in controlling serum magnesium levels. Magnesium deficiency leads to 2.12-fold higher risk of progression to end-stage renal disease (ESRD).
Key words: CKD, dysmagnesemia, magnesium level, prevalence
Author for correspondence: Elvia Jamatia, Assistant Professor, Department of Biochemistry, Dr. Baba Saheb Ambedkar Medical College, Rohini, New Delhi 110085, India. Email: ielvia.j@gmail.com
Received: 21 August 2023; Accepted after revision: 14 April 2024; Published: 13 May 2024
How to cite: Prisi S., et al. Prevalence of dysmagnesemia among CKD patients in North India. J Ren Hepat Disord. 2024;8(1): 17–22.
DOI: 10.15586/jrenhep.v8i1.173
Copyright: Prisi S., et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
The incidence of chronic kidney disease (CKD) is progressively increasing globally. It is important to identify the factors and mechanisms that could obstruct the development of CKD. In this regard, magnesium (Mg) levels have become a critical component that needs to be addressed to decelerate the progression of CKD.
Magnesium is the one of the essential intracellular cations found in the body. It is involved in several biological processes, including signalling pathways, metabolism, cell growth and proliferation, synthesis of macromolecules, such as adenosine triphosphate (ATP), desoxyribonucleic acid (DNA), and ribonucleic acid (RNA) apoptosis and control of cell motility.1 It is also involved in the regulation of sodium and potassium transport. Owing to the involvement of magnesium in various vital molecular processes, the study of magnesium abnormalities has gained interest over the past decade.
The kidneys play a vital role in magnesium homeostasis. Hypomagnesemia has been associated with a number of factors, such as insulin resistance, diabetes, oxidative stress, inflammation, and hypertension, which are thought to contribute to the progression of CKD, according to the data obtained from various experimental and observational studies.2,3 Magnesium is an active regulator for the expression of pro-inflammatory genes and cytokines, such as tumour necrosis factor α (TNF-α), responsible for oxidative stress, and endothelial dysfunction results in promoting renal and cardiac abnormalities. However, several studies found significant association between serum magnesium levels, deterioration in kidney function, and renal outcomes in CKD.4,5 Abnormal homeostasis of magnesium by the kidney leads to either hypermagnesemia or hypomagnesemia and is linked with diverse clinical outcomes that could be fatal. Hence, in this study we investigated the serum levels of magnesium and its association with different stages of CKD.
Material and Methods
It is a retrospective study conducted at the Department of Biochemistry, Maulana Azad Medical College, New Delhi, India, over a period of 2 months (IEC registration No. ECR/329/Inst/DL/2023/RR-2019). Sample size (n) for the study was calculated using the following formula:
n = z2. p.q/d2,
where z = 1.96 at 95% CI, n is the sample size, p is the prevalence of hypomagnesemia in previous studies, q = (1 – p), and d is the margin of error. Taking the prevalence of hypomagnesemia to be 15%, z as 1.96, and margin of error as 5%, the minimum required sample size was 196. In all, 224 patients, receiving treatment at Lok Nayak Hospital, New Delhi, India, participated in this investigative study.
The laboratory data of patients was analysed for statistical relationship between serum magnesium levels and CKD stages. The serum samples were processed on AU480 clinical chemistry analyser (Beckmann Coulter). The blood urea level and serum creatinine level were estimated by enzyme kinetic method and Jaffe’s method, respectively. Serum magnesium level was measured using xylidyl blue by colorimetric method. Serum sodium and potassium levels were estimated using an ion selective electrode indirect method. Serum total calcium levels and serum phosphorus levels were measured using arsenal III method and phosphomolybdate method, respectively. The normal range of serum sodium and serum potassium levels were 136–145 mmol/L and 3.5–5.1 mmol/L, respectively.6 The normal serum total magnesium concentration was 1.8–2.6 mg/dL. We also studied the pattern of serum calcium and serum phosphorus levels with respect to different stages of CKD. The normal reference range of serum total calcium and serum phosphorus were 8.4–10.2 mg/dL and 2.5–4.5 mg/dL, respectively.7
According to the National Kidney Foundation Kidney Disease Outcomes Quality Initiative (NKF KDOQI) guidelines, CKD is defined as either kidney damage or glomerular filtration rate (GFR) < 60 mL/min/1.73 m2 for at least 3 months.7 The worldwide prevalence of CKD is 14%, and the most common causes being hypertension and diabetes mellitus.8 The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, and the patients were categorised into the following five stages according to the Kidney Disease: Improving Global Outcomes (KDIGO): Stage 1: kidney damage with normal or increased GFR (≥90 mL/min/1.73 m2); stage 2: kidney damage with mildly decreased GFR (60–89 mL/min/1.73 m2); stage 3: moderately decreased GFR (30–59 mL/min/1.73 m2); stage 4: severely decreased GFR (15–29 mL/min/1.73 m2); and stage 5: kidney failure (<15 mL/min/1.73 m2).8 The estimated GFR was calculated using the CKD-EPI equation, expressed as a single equation:
GFR = 141 * min (SCr/κ,1) α * max (SCr/κ, 1) - 1.209 * 0.993 age * 1.018 (if female) * 1.159 (if black), where SCr is serum creatinine in mg/dL, k is 0.7 for females and 0.9 for males, α is –0.329 for females and -0.411 for males, min indicates the minimum of Scr/k or 1 and max indicates the maximum of Scr/k or 1.
Statistical analysis of the data was conducted using the IBM SPSS V23 software (Chicago, USA). The age and gender distribution among various CKD stages was assessed using one way ANOVA and Chi square tests, respectively. As our study primarily focused on serum magnesium level variations in CKD patients, one way ANOVA was applied to find association between serum levels of magnesium and CKD stages. Pearson’s correlation test was used to explore the relation between the parameters assessed in the study and serum magnesium levels; P < 0.05 was considered as statistically significant.
Results
Demographic profile of the study population
In the present study, 224 CKD patients were included for analysis. The study population had 12 patients (5.4%) of stage G3a, 20 patients (8.9%) of stage G3b, 70 patients (31.3%) of stage G4, and 122 patients (54.6%) of stage G5. The mean age of the study population was 53.4 + 8.95 years. The mean age of the patients in G3a, G3b, G4, and G5 stages of CKD were 44.2 + 2.8, 44.9 + 6.8, 49.4 + 7.09, and 57.7 + 7.83 years, respectively. The age of patients in G5 stage was significantly higher than the G3a, G3b, and G4 stages (P = 0.001). The mean eGFR of the patients was 17.05 + 13.06 mL/min/1.73 m2 (range = 2–76). In the study population, the prevalence of CKD was more in males (63.4%), compared to females (36.6%). Most of the male patients were of stage G5 (49.3%), followed by stage G4 (33.1%), stage G3b (9.9%), and stage G3a (7.7%). Similar pattern of distribution was observed in female patients: 70.7% were in stage G5, 22% in stage G4, 7.3% in stage G3b, and no patient in stage G3a.
Serum magnesium levels
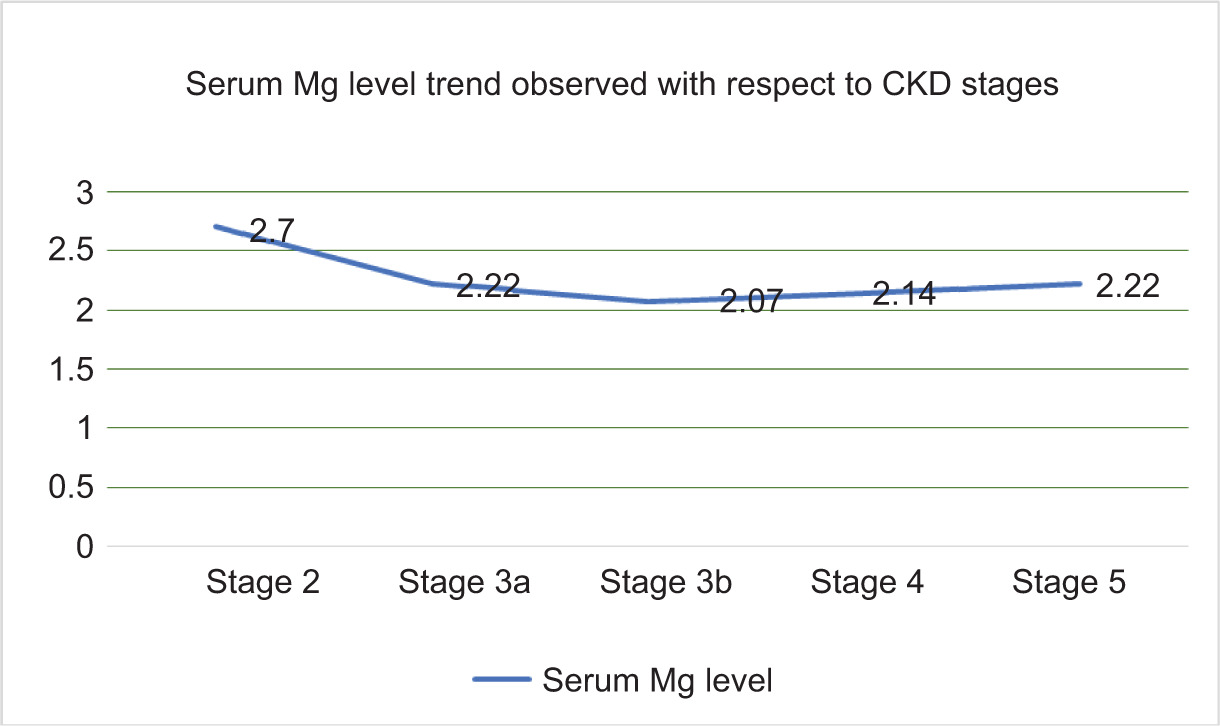
The mean serum magnesium level of the study population was 2.21 + 0.75 mg/dL with a range of 0.32–5.66 mg/dL. Serum magnesium level with respect to CKD stages are shown in Figure 1. The prevalence of hypomagnesemia in the patients was 30.4%, hypermagnesemia was 20.5% whereas 50.9% of the patients were normomagnesemic (with normal level of magnesium ions in the blood). The prevalence of hypomagnesemia decreased from 45% in stage G3 to 28% in stages G4 and G5. Hypomagnesemia was more common than hypermagnesemia (28.0% versus 20.2%) even in the advanced CKD stages of G4 and G5, as shown in Table 2. Hypomagnesemia was the fourth most common electrolyte abnormality across all the stages of CKD. However, no association was found in mean serum magnesium levels among various CKD stages (P = 0.45), as shown in Table 3. Also, no significant correlation was found between serum magnesium levels and blood urea (r = 0.073), serum creatinine (r = 0.02), serum sodium (r = -0.023), serum potassium (r = 0.071), and eGFR (r = 0.02), as shown in Table 4.
Table 1: Demographics and baseline characteristics of the study population (n = 224).
| Mean | Standard deviation (SD) | Min–Max | |
|---|---|---|---|
| Age (years) | 53.4 | 8.95 | 38–78 |
| Baseline renal function parameters | |||
| Urea (mg/dL) | 151.9 | 67.40 | 19–414 |
| Creatinine (mg/dL) | 5.144 | 2.73 | 1.3–15.9 |
| Sodium (mmol/L) | 137.15 | 9.80 | 110–179 |
| Potassium (mmol/L) | 4.49 | 1.03 | 2.7–8 |
| eGFR (mL/min) | 17.05 | 13.06 | 2–76 |
| Baseline serum magnesium parameter (mg/dL) | 2.21 | 0.75 | 0.32–5.66 |
eGFR: estimated glomerular filtration rate.
Figure 1: Trend of serum magnesium level observed with respect to chronic kidney disease (CKD) stages.
Table 2: Distribution of electrolyte panel among CKD patients.
| CKD stages 1, 2, and 3 | CKD stages 4 and 5 | Overall | |||
|---|---|---|---|---|---|
| Prevalence (%) | Prevalence (%) | Prevalence (%) | |||
| Hypocalcemia | 28 (90.3) | Hypocalcemia | 152 (78.8) | Hypocalcemia | 180 (80.4) |
| Hyperphosphatemia | 21 (67.7) | Hyponatremia | 81 (42) | Hyperphosphatemia | 111 (49.6) |
| Hypomagnesemia | 14 (45.2) | Hypomagnesemia | 54 (28) | Hyponatremia | 92 (41.1) |
| Hyponatremia | 11 (35.5) | Hyperkalemia | 44 (22.9) | Hypomagnesemia | 68 (30.4) |
| Hypokalemia | 7 (22.6) | Hypermagnesemia | 39 (20.22) | Hyperkalemia | 50 (22.3) |
| Hypermagnesemia | 7 (22.6) | Hypokalemia | 18 (9.4) | Hypermagnesemia | 46 (20.5) |
| Hyperkalemia | 6 (19.4) | Hypernatremia | 12 (6.2) | Hypokalemia | 25 (11.2) |
Table 3: Association of serum magnesium (median as cutoff: 2.11) and other serum renal parameter.
| Mg < 2.11(n = 113) | Mg > 2.11(n = 111) | P value* | |
|---|---|---|---|
| Urea (mg/dL) | 143.5 + 68.2 | 160.4 + 65.7 | 0.061 |
| Creatinine (mg/dL) | 4.88 + 2.4 | 5.4 + 2.95 | 0.145 |
| Sodium (mmol/L) | 136.9 + 8.11 | 137.3 + 11.3 | 0.72 |
| Potassium (mmol/L) | 4.3 + 0.98 | 4.6 + 1.06 | 0.11 |
| eGFR (mL/min) | 17.9 + 13.0 | 16.11 + 13.1 | 0.28 |
*Independent t-test of significance.
eGFR: estimated glomerular filtration rate.
Table 4: Pearson’s correlation of serum magnesium with other serum renal parameters.
| Urea | Creatinine | Na | K | eGFR | |
|---|---|---|---|---|---|
| Mg | 0.073 | 0.020 | –0.023 | 0.071 | 0.02 |
eGFR: estimated glomerular filtration rate.
Serum sodium, potassium, calcium, and phosphorus levels
The mean serum level of sodium was 137.15 ± 9.8 mmol/L, serum level of potassium was 4.49 ± 1.03 mmol/L, serum level of calcium was 7.70 ± 0.92 mg/dL, and serum level of phosphorus was 4.56 ± 1.13 mg/dL. Overall, hypocalcemia (80%) was the most common electrolyte disorder, followed by hyperphosphatemia (50%), hyponatremia (41%), and hypomagnesemia (30%), as shown in Table 2.
Serum creatinine and blood urea levels
The mean blood urea level in the study population was 151.9 + 67.4 mg/dL (range = 19–414 mg/dL) and serum creatinine level was 5.14 + 2.73 mg/dL (range = 1.3–15.9 mg/dL).
Discussion
The homeostasis of magnesium mainly depends on the balance between its intestinal absorption and renal excretion. A progressive decline in renal function and retention of uraemic solutes were observed with CKD progression. If GFR < 30 mL/min, then urinary magnesium excretion is not able to balance its intestinal absorption, and the responsibility of magnesium homeostasis solely depends on dietary intake.9 Even though renal failure is a leading cause of raised magnesium levels, the resulting hypermagnesemia is generally mild and asymptomatic, even in ESRD patients.
As multiple factors are involved in controlling serum magnesium levels in progressive CKD and ESRD patients, some of these factors produce a negative magnesium balance as well. Some such conditions are massive consumption of diuretics, decreased gastrointestinal absorption (owing to acidosis, poor dietary intake, and absorption), and inadequate magnesium concentration of dialysate.10 In the present study, the prevalence of hypomagnesemia in stages G3, G4, and G5 pre-dialysis CKD patients was 30% whereas the prevalence of hypermagnesemia in the study population was 21%. This was a deviation from the fact that in the setting of low GFR and insufficient renal excretion, hypomagnesemia should be rare. However, as found in few studies, in spite of reduced GFR in CKD patients, hypomagnesemia was not infrequent among them. Similar results were observed by Kotha et al. in the south Indian population with an overall prevalence of 21.6% hypomagnesemia and 10.8% hypermagnesemia in CKD patients.11 The authors discovered mean serum magnesium as 2.02 ± 0.36 mg/dL in study patients and 2.01 ± 0.17 mg/dL in controls of their study population, which was not statistically significant.11 Oka et al, found that hypomagnesemia was one of the most prevalent dyselectrolytemia (imbalance in the required amount of electrolytes, such as calcium, potassium, sodium, and magnesium in the blood) among CKD patients, which was almost 15% even in stages G4 and G5.12 Similar results were discovered by Sakaguchi et al., with hypomagnesemia to be a common electrolyte disorder in pre-dialysis CKD patients.13
The underlying processes involved in the development of hypomagnesemia in CKD patients were varied. For instance, limited intake of potassium in diet could restrict the magnesium intake, as potassium-rich foods are also a rich source of magnesium. Inadequacy in magnesium excretory pathways is the primary cause of renal loss of magnesium. These could be a result of either inherited or acquired conditions. The inherited disorders associated with urinary magnesium wasting include conditions such as familial hypomagnesemia with hypercalciuria and nephrocalcinosis (FHHNC), Bartter syndrome, and Gitelman syndrome. Medications, such as diuretics, and alcohol are mainly responsible for acquired hypomagnesemia. Loop and thiazide diuretics inhibit electrical gradient and thereby affect net magnesium reabsorption in the thick ascending loop. Potassium-sparing diuretics could be a better choice, because by increasing magnesium transport, it lowers the excretion of magnesium.10 Certain nephrotoxic drugs, such as aminoglycoside antibiotics, amphotericin B, cisplatin, pentamidine, tacrolimus, and cyclosporine, result in hypomagnesemia by decreasing loop and distal magnesium reabsorption. Alcohol-induced tubular dysfunction, leading to excess of urinary excretion of magnesium, with a prevalence of around 30%, is another commonly experienced condition.9 Apart from these, hypercalcemia also causes hypomagnesemia by a compensatory decrease in magnesium reabsorption because of increased filtered calcium load to the loop of Henle. Serum magnesium level is affected by both hypercalcemia and hypocalcemia.7 Hypocalcemia is also a common manifestation in hypomagnesemia, however symptomatic only in patients with moderate to severe magnesium deficiency. Different mechanisms are hypothesized for hypocalcemia associated with magnesium deficiency such as impaired secretion of parathyroid hormone (PTH), end-organ resistance to PTH, increase in PTH metabolism, decrease in 1,25 dihydoxyvitamin D (calcitriol), etc.10 However, it is resistant to correction with calcium, vitamin D, or both; however, magnesium therapy alone could improve hypocalcemia.
Renal failure, including ESRD patients, remains the most common cause of hypermagnesemia, usually mild and asymptomatic. As CKD patients need dialysis at some point of management, studies have shown increased bone magnesium by 66% in both cortical and trabecular bones. Dietary magnesium intake becomes major determinant of serum and total body magnesium levels with CKD progression because urinary magnesium excretion fails to counterbalance intestinal magnesium absorption. Complication arises with administration of magnesium-containing drugs (e.g., antacids and laxatives), and dialysate with high magnesium concentration could induce severe, symptomatic, or even fatal hypermagnesemia. Progressive decrease in kidney function is accompanied by retention of uraemic solutes and increased mortality risks.
In a study conducted by Takayanagi et al. with mice with unilateral ureter obstruction, the ureter-ligated kidney showed a dramatic drop in claudin-16 and transient receptor potential M6 with upregulation of claudin-14.14 After the release of ureteral ligation, significant decrease in serum magnesium levels accompanied by an increased fractional excretion of magnesium was observed.15 Oka et al. found a positive correlation between fractional excretion of magnesium and tubular injury markers, such as β2-microglobulin, in non-dialysis CKD patients, which was consistent with previous studies conducted on animals.12
Progression of CKD is affected by magnesium deficiency, as supported by a retrospective cohort study, which showed 2.12-fold higher risk of progression to ESRD (95% CI 1.28–3.51; P = 0.004) in CKD patients with hypomagnesemia.9 Low-magnesium diet for 6 weeks for hemi-nephrectomized CKD model mice down-regulated α-klotho expression in the kidney with aggravated tubular injury and interstitial fibrosis induced by high-phosphate diet. Underlying pathophysiology for phosphate-induced cell death was magnesium-attenuated mitochondrial dysfunction and inflammation of proximal tubular cells, as supported by a cohort study comprising non-diabetic CKD patients. The study also discovered that risk was mitigated if their serum magnesium levels were high, and this concept could be useful to prevent phosphate-induced kidney injury.9
Magnesium plays a crucial role in regulating arterial blood pressure by increasing nitric oxide synthesis and reducing total peripheral resistance. It also helps in maintaining physiological health via antithrombotic action (inhibits upregulation of PAI-1), anti-inflammatory response, and by facilitating re-endothelialization of vascular injuries.16 Thus, hypomagnesemia is a possible participant in the development of cardiovascular diseases in the population and its supplementation could improve clinical outcomes by preventing the progression of vascular calcification.4
In a cohort study comprising 142,555 haemodialysis patients from the Japanese Society for Dialysis Therapy–Renal Data Registry, it was observed that serum magnesium level affected the mortality rate. While mild hypermagnesemia (2.7–3.0 mg/dL) showed improved survival, high mortality rate was associated with low pre-dialysis serum magnesium levels as well as serum magnesium levels of ≥3.1 mg/dL.9 Some confounding factors, such as nutritional status or medical supplementation of magnesium oxide, and management of dialysis patients may have a role in mild hypermagnesemia and better survival. Further, well-designed randomised trials are required to determine optimal serum magnesium levels in haemodialysis patients.
Conclusions
Compelling evidence supports the clinical significance of magnesium among CKD patients with respect to vascular calcification and mortality. However, many of the underlying mechanisms, such as target range of serum magnesium levels and the best approach to increase serum magnesium levels, still remained to be explored. Besides, there is a need to develop an effective management for refractory hypomagnesemia. More randomised trials are required to find solutions and establish an optimal strategy for managing CKD patients with hypomagnesemia for better prognosis.
Prior presentation: 2nd prize awarded in oral presentation at the CME on “An insight into Diabetes Mellitus and an update on its various complications” organized by the Department of Biochemistry, Dr. Baba Saheb Ambedkar Medical College, Rohini, New Delhi, on 14 November 2022.
Acknowledgement
Department of Biochemistry, Maulana Azad Medical College, New Delhi, India.
REFERENCES
1. Romani AMP. Magnesium homeostasis in mammalian cells. Front Biosci J Virtual Libr. 2007;12:308–31. 10.2741/2066
2. Kostov K. Effects of magnesium deficiency on mechanisms of insulin resistance in type 2 diabetes: Focusing on the processes of insulin secretion and signaling. Int J Mol Sci. 2019;20:1351. 10.3390/ijms20061351
3. Severino P, Netti L, Mariani MV, Maraone A, D’Amato A, Scarpati R, et al. Prevention of cardiovascular disease: Screening for magnesium deficiency. Cardiol Res Pract. 2019;2019:4874921. 10.1155/2019/4874921
4. Massy ZA, Drüeke TB. Magnesium and cardiovascular complications of chronic kidney disease. Nat Rev Nephrol. 2015;11:432. 10.1038/nrneph.2015.74
5. Nielsen FH. Magnesium deficiency and increased inflammation: Current perspectives. J Inflamm Res. 2018;11:25–34. 10.2147/JIR.S136742
6. Schindler EI, Brown SM, Scott MG. Electrolytes and blood gases. In: Teitz fundamentals of clinical chemistry 6th ed, Chap. 35.
7. Felsenfeld AJ, Levine BS, Rodriguez M. Pathophysiology of calcium, phosphorus, and magnesium dysregulation in chronic kidney disease. Semin Dial. 2015 Nov;28(6):564–77. 10.1111/sdi.12411
8. Kidney International. Definition and classification of chronic kidney disease: A position statement from kidney disease: Improving global outcomes (KDIGO) [Internet]. [cited 2022 Mar 27]. Available from: https://www.kidney-international.org/article/S0085-2538(15)50698-4/fulltext
9. Navarro-González JF, Mora-Fernández C, García-Pérez J. Clinical implications of disordered magnesium homeostasis in chronic renal failure and dialysis. Semin Dial. 2009;22:37–44. 10.1111/j.1525-139X.2008.00530.x
10. Martin KJ, González EA, Gellens ME, Hamm LL, Abboud H, Lindberg J. Therapy of secondary hyperparathyroidism with 19-nor-1alpha,25-dihydroxyvitamin D2. Am J Kidney Dis. 1998;32(2 Suppl 2):S61–6. 10.1053/ajkd.1998.v32.pm9808145
11. Kotha NB, Ganesh M, Manikandan A, Selvarajan S, Muthukathan R. Serum magnesium levels in chronic kidney disease patients. Sri Ramachandra J Health Sci (SRJHS). 2022 Jul 15;2(1):29–32.
12. Oka T, Hamano T, Sakaguchi Y, Yamaguchi S, Kubota K, Senda M, et al. Proteinuria-associated renal magnesium wasting leads to hypomagnesemia: A common electrolyte abnormality in chronic kidney disease. Nephrol Dial Transplant. 2019;34:1154–62. 10.1093/ndt/gfy119
13. Sakaguchi Y, Hamano T, Kubota K, Oka T, Yamaguchi S, Matsumoto A, et al. Anion gap as a determinant of ionized fraction of divalent cations in hemodialysis patients. Clin J Am Soc Nephrol (CJASN). 2018 Feb 7;13(2):274–81. 10.2215/CJN.07930717
14. Sakaguchi Y. The emerging role of magnesium in CKD. Clin Exp Nephrol. 2022 Jan;26(5):379–384. 10.1007/s10157-022-02182-4
15. Takayanagi K, Shimizu T, Tayama Y, Ikari A, Anzai N, Iwashita T, et al. Downregulation of transient receptor potential M6 channels as a cause of hypermagnesiuric hypomagnesemia in obese type 2 diabetic rats. Am J Physiol Renal Physiol. 2015 Jun 15;308(12):F1386–97. 10.1152/ajprenal.00593.2013
16. Turgut F, Kanbay M, Metin MR, Uz E, Akcay A, Covic A. Magnesium supplementation helps to improve carotid intima media thickness in patients on hemodialysis. Int Urol Nephrol. 2008 Dec;40(4):1075–82. 10.1007/s11255-008-9410-3