
Download

Review
An update on current clinical pathogenesis, prevention, and nutritional aspects of nephrolithiasis: a review
Pranjal Sachan1,*, Anjali Pandey2
1Department of Pharmaceutics, Sanskriti College of Higher Education and Studies, 209111 Bhognipur, India
2Department of Pharmacology, Shambhunath Institute of Pharmacy, 211015 Prayagraj, India
Abstract
Nephrolithiasis, commonly known as kidney stone disease, is a prevalent condition characterized by the formation of hard crystalline deposits within the renal system, primarily due to metabolic abnormalities in urinary composition. In India, the prevalence of urinary stone disease is estimated to be around 12%, with a significant proportion at risk of progressing to renal impairment if left untreated. This review explores both pharmacological and nutritional strategies for the prevention and management of recurrent kidney stones. A comprehensive literature search was conducted using databases such as PubMed and Google Scholar, and major publishers including Springer Nature, Bentham Science, Taylor & Francis, and Elsevier. Pharmacological interventions such as thiazide diuretics, indapamide, allopurinol, and potassium citrate have been shown to reduce urinary calcium and uric acid levels, thereby mitigating stone formation. In parallel, several medicinal plants, including Asparagus racemosus, Virataradigana, and Boerhaavia diffusa, exhibit diuretic and antiurolithiatic properties and have shown promising outcomes in traditional medicine and preliminary clinical studies. Although the pharmacological agents demonstrate well-established mechanisms of action and clinical efficacy, the supportive role of herbal remedies offers a complementary pathway, particularly in populations with limited access to conventional therapies. However, the current body of clinical evidence for herbal therapies remains limited in scope and rigor. Thus, while the combined approach of pharmaceutical and plant-based interventions offers a comprehensive strategy for reducing stone recurrence and preserving renal function, further large-scale, randomized clinical trials are necessary to validate these findings and to establish standardized protocols for effective nephrolithiasis management.
Keywords: Renal stones; Calcium oxalate crystals; Urinary stones; Pharmacological treatment; Non-pharmacological treatment; Herbal plants; Clinical trials
Submitted: 30 November 2024; Accepted: 17 July 2025; Published: 20 December 2025
Authors for correspondence: Emails: pranjupsit@gmail.com
How to cite: Pranjal Sachan, Anjali Pandey. An update on current clinical pathogenesis, prevention, and nutritional aspects of nephrolithiasis: a review. Journal of Renal and Hepatic Disorders. 2025; 9(2): 1-21. doi: 10.63268/jrenhp.v9i2.210.
Copyright: The Author(s). Published by Troika Publisher. License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
Hard accumulations are made of substances such as salts and minerals called kidney stones that form inside your kidneys. They are also known as nephrolithiasis, renal stones, or urolithiasis. Kidney stones are most common in people between 30 and 60. Men are more impacted than women by discomfort that is intense and caused by renal colic, a kidney stone, is expected to affect 3–5% of women and 10–20% of men. Throughout India, 12 percent of persons are predicted to develop urinary stones, and then 50% of those situations might lead to kidney loss and renal impairment [1]. Future kidney stone incidence is predicted to rise as a result of lifestyle modifications, food alterations, and obesity [2, 3].
Kidney stone disease imposes a substantial economic burden, attributed to the high costs of medical interventions and productivity loss resulting from work absenteeism [4]. It is associated with a higher prevalence of raised blood pressure, myocardial infarction, as well as chronic kidney disease [5, 6, 7]. The most common Escherichia coli (E. coli) causes urinary tract infections (UTIs), accounting for the majority of cases in both community and healthcare settings.
There are no preliminary signs of the stone formation. Subsequently, kidney stones (acute cramps illness), flank ache (back discomfort), haematuria (blood-soaked urine, pulmonary), (urethral disorder), infection of the urinary tract, and obstructions to urine flow, and signs of stone disease include pyelectasis or pelviectasis (Urinary tract dilation) [8].
Urolithiasis prevalence has grown internationally in recent decades, with figures ranging from 4.7% in Germany, 10.1% in America [9]. Stones in the bladder have a significant recurrence rate, estimated to be more than 50% after ten years. Nephrolithiasis has been linked to an increased likelihood of chronic as well as advanced kidney disease, which is probably due to kidney damage induced by obstructive kidneys [10].
The most common kind of stone is calcium oxalate (67%), preceding calcium phosphate (17%), uric acid (8%), struvite (3%), as well as cystine (0.4%) [11]. Urinary stone development is a complicated process that can be influenced by metabolic derangements, hereditary variables, anatomical and functional abnormalities, and diet is important [12]. Dietary composition can influence urine dangers oversaturation alongside stone-forming salt, altering the potential danger of urinary stone development [13].
Due to urinary indicators of danger for stone development differing depending on the kind of stone, a reliable stone analysis is required before beginning particular treatment regimens. Furthermore, the stone patient must have a full metabolic examination, which includes a detailed medical history, nutritional assessment, and analysis of the stools and blood [14]. To lower the likelihood of recurring stone development, focused nutritional therapy ought to be customised for each individual metabolic risk profile [15].
Two consecutive 24-hour urine samples are indicated for detecting frequent metabolic abnormalities. These abnormalities include hypercalciuria, hypocitraturia, hyperoxaluria, and hyperuricosuria. They are also useful for recognising dietary risks for kidney stone development [16]. Based on dietary and metabolic assessments, specific nutritional treatment is generally more effective than wide dietary guidelines in avoiding continuous granite construction. The purpose of the following narrative examination summarizes current understanding about the significance of diet kidney stones.
Urinary system and stones
The glomerulus creates urine filtrate, which eventually goes through the tubules, whereby reabsorption or secretion alter the volume and content. The previously proximal tubules absorb the majority of solutes, whereas the distal tubules, including collecting ducts, make little changes to urine composition.
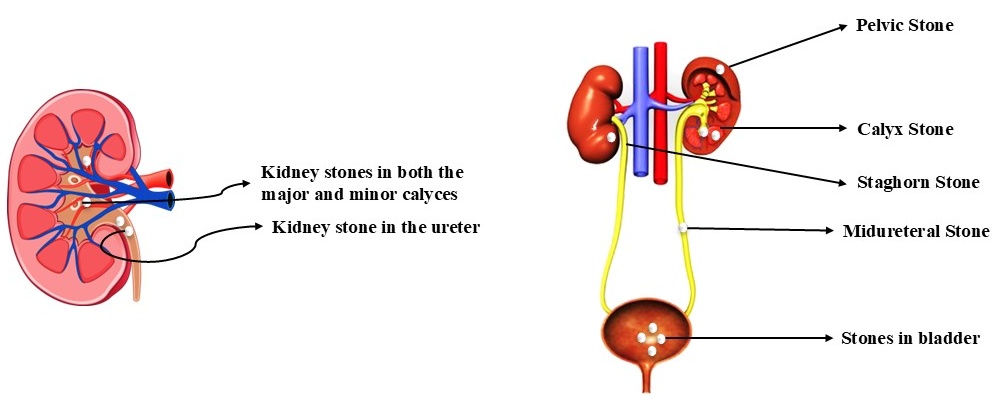
The necessary components, including protein, amino acids, bicarbonate, calcium, phosphate, and potassium, are all reabsorbed either returned to the body circulatory system through proximal tubes in conjunction with glucose, sodium chloride, chloride, in addition water [17], as shown in the Fig. 1, Ref. [18]; Fig. 2, Ref. [18].
Figure 1 Location of a kidney stone in the urinary system [18].
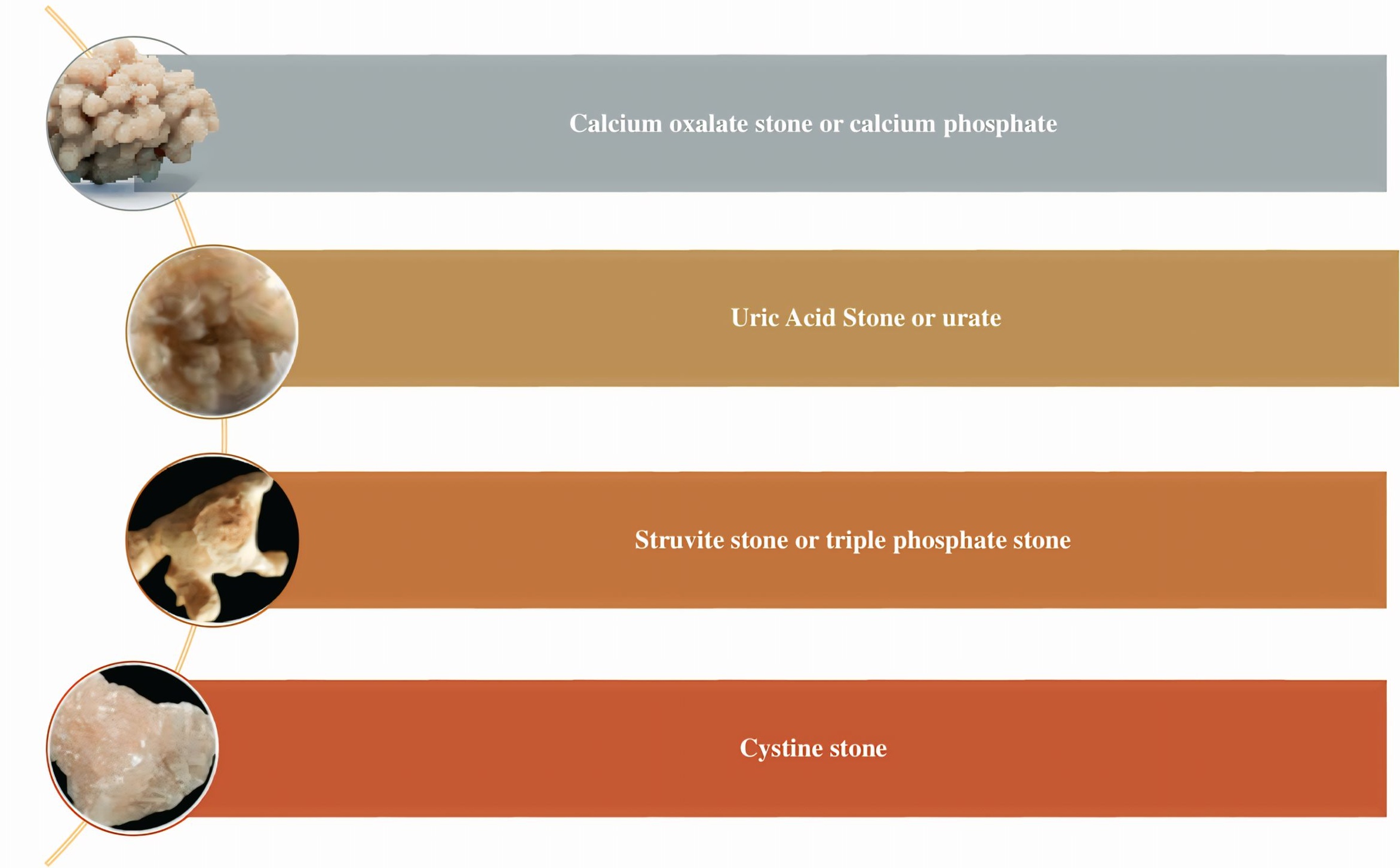
Figure 2 Different types of kidney stones [18].
Calcium stone contains calcium phosphate together with oxalate
Most urinary stones (around 80%) are calcium stones, which predominate among renal stones [19]. 50 The majority of calcium stones consist of calcium oxalate (CaOx) as well as calcium phosphate (CaP), commonly referred to as apatite. Each factor individually accounts for 5 percent, and collectively they contribute 45 percent [20].
Struvite stones or magnesium ammonium phosphate rocks
These material stones, additionally referred to as infectious acute triple phosphate stones, are primarily linked to infection of the urinary tract produced by bacteria that generate urease, such as Proteus mirabilis, Klebsiella, among Pseudomonas. These microbes convert urea to ammonia, raising urine pH and aiding the precipitation of calcium, magnesium ammonium phosphate. Struvite stones may account for 10–15% of all kidney-related stone cases, particularly in people who have frequent urinary tract infections (UTIs).
Uric acid stone or urate
Urinary acid stones represent about 8–10% of all renal calculi. They are commonly associated with conditions that cause increased purine metabolism, such as diets high in animal proteins (meat and fish), obesity, and gout. Hyperuricosuria (excess uric acid in urine) and persistently acidic urine (pH <5.5) promote the crystallization producing uric acid, resulting in stone formation. Individuals with metabolic syndrome and chronic dehydration are also at elevated risk.
Cystine stones
Below 2%, including all stone kinds are these stones. It is a hereditary condition that affects how an organic compound or cystine is transported. It causes an overabundance of cystinuria, an autosomal recessive disorder characterized by defective cystine tube absorption, especially cystine leakage into the urine, and is brought on by a genetic deficiency in the natural and basic amino acid transport protein gene located on a chromosome [21]. It causes the production of cystine stones because it is not released in urine, as indicated in Table 1 [13, 14, 15].
Table 1: Risk considerations for stone formation.
| Disease | Threat factor |
|---|---|
| Hypercalcemic disorders | Primary hyperparathyroidism as well as other calcium metabolism issues. |
| Recurrent urinary tract infections | Aberrant urine pH and urine that has been alkalinized by bacteria that produce urease, including Proteus mirabilis. |
| Metabolic disorders | That includes a history of gout (a form of uric acid metabolism disorder), hypercalciuria, hypocitraturia, hyperoxaluria, as well as hyperuricosuria. |
Pathophysiology of kidney stones
As per their chemical components, kidney stones are categorized. Many solutes inside the urine may crystallize, followed by lithogenesis [22] (Table 2). Urine must have been supersaturated concerning the substance of the stone, which means the required concentration must be greater compared to the material’s thermodynamic solubility, for crystal formation.
Table 2: Main causes of calcium stone formation.
| Disease | Definitions | Etiology |
|---|---|---|
| Hypercalcinuria | Excessive urinary calcium excretion 200 mg/d | Absorbent hypercalcinuria: Enhance the urinary absorption of calcium in the digestive system. Hypercalcemia: Impairment of the kidneys, Resorptive. Hypercalciuria: Initial hyperparathyroidism. |
| Hyperoxaluria | Excessive oxalate levels in urine 40 mg/d | First-stage hyperoxaluria: Genetics of oversupply of Oxalate and nutrients. Hyperoxaluria: Excess amount of food consumption causes. Entrance hyperoxaluria: Absorption of gastrointestinal oxalate. |
| Hypocitraturia | Citrate is eliminated in the urine at a rate of 320 mg per day, significantly less | Distal tubular hyperkalemia: Reduced acidic expels from the renal tubules. Chronic diarrhea syndrome: Associated with gastrointestinal (GI) enzyme deficiency. Thiazide-induced: Hypokalaemia. |
| Hyperuricosuria | High uric acid levels in the urine, 600 mg/d | Increased uric acid synthesis, dietary excretion, and urine production. |
Pathogenesis and mechanism of kidney stone formation
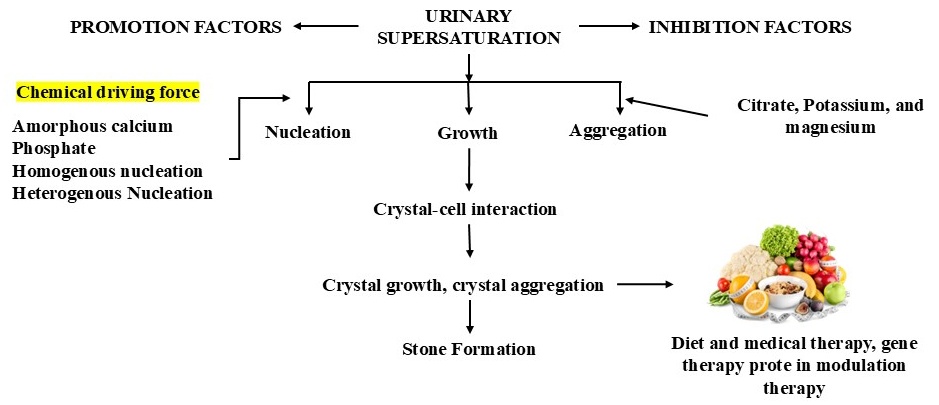
Urine must release crystalloids that can form stones for renal stones to develop. With calcium oxalate and phosphate combined, calcium serves as the primary constituent of more than 75 percent of all gravels. Several stages, like calcium oxalate (CaOx) or calcium phosphate build-up, occur during calcium stones (CAP) production [23], as shown in the Fig. 3 (Ref. [24]).
Figure 3 An illustration showing how calcium oxalate kidney stone development is induced and inhibited [24].
This procedure is encouraging the production of stones.
• Urinary supersaturation.
• Crystals nucleation.
• Crystals accumulation.
• Crystals retain.
Urinary supersaturation and crystallization
The cause of crystal growth in the kidneys is urinary supersaturation. Supersaturation is unquestionably necessary for stone synthesis since it’s important for the initiation of the development of crystalline particles [25].
Crystal nucleation
When a supersaturated solution changes from a state of fluid to a solid phase, the process is referred to as nucleation [26].
Crystals developing
After the crystal’s nucleus approaches an appropriate dimension and comparative excessive saturation has passed, adding more crystal components causes the total free energy to decrease [27].
Crystals accumulation
When minerals in the resolution work together to produce bigger particles, the process is termed agglomeration. According to several studies, crystal gathering is the critical stage in the production of stones. Although crystal development is undoubtedly a phase in the creation of CaOx renal stone, crystals develop at a sluggish rate.
Integrated approaches for the management of kidney stones: pharmacological and non-pharmacological strategies
The management of kidney stones encompasses a comprehensive spectrum of pharmacological and non-pharmacological interventions aimed at both treating existing calculi and preventing recurrence Fig. 4 (Ref. [28]). Pharmacological treatments primarily focus on modifying the biochemical environment of the urine to inhibit stone formation or aid in stone dissolution. Agents such as thiazide diuretics are commonly used to reduce urinary calcium excretion in patients with calcium-containing stones, while potassium citrate is frequently administered to alkalinize urine and prevent the crystallization of uric acid and cystine stones. Allopurinol, a xanthine oxidase inhibitor, is prescribed in hyperuricosuric patients to lower uric acid levels. Additionally, magnesium supplements and phosphate salts may be used to stabilize urinary constituents and prevent stone aggregation [29].
Figure 4 Overview of pharmacological and non-pharmacological strategies for the management of kidney stones [28].
On the other hand, non-pharmacological strategies play a vital role in long-term stone prevention and include dietary modifications, adequate hydration, and lifestyle adjustments. Increasing fluid intake to maintain a urine output of at least 2 to 2.5 liters per day is a foundational recommendation, as it dilutes urinary solutes and reduces supersaturation. Dietary interventions emphasize reducing the intake of oxalate-rich foods, sodium, and animal proteins while ensuring adequate calcium intake from dietary sources to bind oxalates in the gut. Lifestyle modifications such as maintaining a healthy body weight and engaging in regular physical activity have also been associated with reduced stone risk [30]. Together, these integrative approaches underscore the importance of individualized, patient-centered management plans that address both the biochemical and behavioral aspects of kidney stone disease, thereby improving clinical outcomes and minimizing recurrence rates.
Pharmacological treatment of kidney stones
Urine production should be at least 1/2 day; therefore, intake of fluids should be enough. Patients with moderate-to-severe stone disease should be the only ones who take medications. There is the various pharmacological treatments for kidney stones.
Hypercalciuria
Hypercalciuric nephrolithiasis has frequently been treated with hypocalciuric action. These drugs are specifically approved for treating renal hypercalciuria because they target the urinary tract, where they directly increase calcium reabsorption in the renal tubules. However, they are also often used in absorptive hypercalciuria with acceptable management of hypercalciuria [31].
Indapamide
Although it has the capability to treat hypercalciuria, indapamide can also cause hypokalaemia and hypocitraturia. It can be administered once daily (2.5 mg/day) as a long-acting diuretic. For the best hypercalciuria management with hypocalciuric medicines, sodium intake from food should be limited to a lower than 100 mEq/day. Over potassium chloride, potassium citrate is recommended [32].
Hypocitraturia
Hypocitraturia (150 mg/day) typically denotes conditions characterized by a significant level of acid or acidic conditions, such as proximal renal tubular acidosis, persistent diarrhea, severe exercise, or topiramate medication.
Hyperoxaluria
The limitation of dietary oxalate and an increase in fluid consumption are essential. Potassium citrate might be used for the treatment of associated hypocitraturia and low urine pH in chronic diarrheal conditions accompanied by moderate-severe hyperoxaluria [33].
Calcium citrate (500 mg calcium bi-daily) may treat calcium shortage and reduce urinary oxalate when urine calcium levels are low [34].
Hyperuricosuria
Allopurinol may be recommended for severe hyperuricosuria (>850 mg/day) or to coexist with hyperuricemia.
Allopurinol
By deactivating xanthine oxidase, this substance suppresses the transformation of xanthine into uric acid. In the majority of people who develop stones, each day, 300 mg of allopurinol can be taken to obtain appropriate treatment for hyperuricemia or hyperuricosuria [35, 36, 37] (Table 3, Ref. [38, 39, 40, 41, 42]).
Table 3: Kidney stones and their effect or treatment in human studies.
| No. | Study Author | Treatment | Effect | Result |
|---|---|---|---|---|
| 1 | Malihi Z et al. [38] 2020 | Hypercalciuria | Patients with hypercalciuria are more likely to experience osteoporosis-causing bone loss. | The baseline dose and duration of 25-hydroxyvitamin D co-supplementation did not affect the relationship between vitamin D intake and the risk of either hypercalciuria causing kidney stone development. |
| 3 | Ceylan K et al. [39] 2016 | Indapamide | In individuals with high urine calcium concentrations, it is efficient and advised for the prevention of recurring calcium stones. | Median parathyroid hormone, potassium levels, and diastolic and systolic blood pressure measurements were all significantly lower than expected. Serum uric acid and levels of triglycerides were significantly elevated. |
| 4 | Shabani Nashtaei M et al. [40] 2019 | Hyperoxaluria | When a person has hyperoxaluria, their urine contains excessive amounts of oxalate, a substance that can cause kidney stones. | Researchers demonstrated that the existence of O. formigenes might decrease the development of 24-hour urine oxalate and its function in hyperoxaluria, although it may not necessarily be caused by kidney stone illness. |
| 5 | Spivacow FR et al. [41] 2016 | Hyperuricosuria | Rising uric acid output in the urine and calcium stone illness. | When untreated and even after uric acid production has been reduced with a xanthine dehydrogenase inhibitor like allopurinol, hyperuricosuria frequently causes the development of stones in the nephrocalyceal medullae, or known as the urological system. |
| 6 | Astroza GM et al. [42] 2016 | Hypocitraturia | Citrate prevents the formation of stones by preventing the nucleation, proliferation, and crystallization of calcium in the urine. | Between 20% and 60% of the stones in the kidney form have hypocitraturia, a common metabolic disorder. It denotes a low concentration of the acid in the urine. |
Potassium citrate
The addition of potassium citrate could be an option for people who have a rise in urine uric acid of mild to moderate severity (600–850 mg/day) or who have allopurinol adverse effects Table 4 [36].
Table 4: Pathophysiological conditions and mechanisms of kidney stone formation.
| Condition | Drug | Dose | MOA |
|---|---|---|---|
| Renal hypercalciuria | Indapamide | 4 mg | ↑ Reabsorption of renal calcium |
| Hypocitraturia | Potassium Citrate | 20 mg | ↑ Urinary citrate ↓ Urinary calcium |
| Hyperoxaluria | Potassium Citrate | 20 mg | ↑ Urinary citrate ↓ Urinary oxalate |
| Hyperuricosuria | Allopurinol | 20–30 mg | ↓ Serum and urinary uric acid |
MOA: Mechanism of action. ↑ indicates increase; ↓ indicates decrease.
Non-pharmacological treatment of kidney stones
Asparagus racemosus
The plant Asparagus racemosus, also referred to as Shatavari or shatamuli, is a member of the Asparagaceae family. The roots of the plant, dried, exhibited galactagogue, antitussive, antibacterial in nature, antisecretory, anti-ulcer, anti-protozoal, anti-hepatotoxic, antioxidants, antineoplastic, adaptogenic, antilithiatic activities, among other properties [42].
Viratarvadigane
The Amaranthaceae family includes Viratarvadigana, also known as Celosia argentea. The leaves and stems of the plant are used to cure urinary problems, eye problems, diarrhea, and sore mouth [43].
Boerhaavia diffusa
The Nyctaginaceae family includes Boerhaavia diffusa, which is additionally known as Punarnava herb, Santhi, Sanadika, Gonajali, Sanadika, Sothaghna, and other names. Punarnava serves as a kidney treatment and assists in the expulsion of kidney stones; hence, it is advised for those with renal and urinary illnesses [44].
Tribulus terrestris
A member of the Zygophyllaceae family, Tribulus Terrestris is commonly referred to as Gokshura or Tribulus. Roots and fruits of Tribulus Terrestris help treat stones in the kidneys, impotence, and painful urinary tract infections [45].
Phyllanthus niuri
The plant Phyllanthus niruri, often called Chanca piedra or stonebreaker, is a member of the Euphorbiaceae family. Phyllanthus niruri compounds act against fungi, bacteria, inflammation, hyperglycemia, analgesia, hepatoprotection, and lithiasis [46].
Ammi visnaga
A member of the Apiaceae family is Ammi Visnaga, also known as Khella. People with kidney stones have traditionally used a variety of teas brewed from the vegetables and fruits of A. visnaga [47].
Crataeva nurvula
A member of the Capparidaceae family, Crataeva nurvala is commonly referred to as Varuna bark and Varuna. According to research, the main ingredient in C. nurvala, lupeol, inhibits the enzyme glycolate oxidase, reducing the body’s production of oxalates [48].
Oenothera biennis
The plant Oenothera biennis, sometimes known as evening primrose, is a member of the Onagraceae family. By suppressing lipogenesis and increasing the level of citrate in the urine while lowering oxalate concentration in urine by changing the membrane fatty acids, daily use of primrose in the evening renal stones by lowering risk by 1000 mg/day of seed oil intake [49].
Prevention of kidney stones
A low-cost public health project with significant social repercussions is the primary prevention of the formation of stones in their kidneys by diet modification.
The greatest way to avoid urolithiasis is through dietary control [50]. Patients should be told to drink more water so they can keep their urine production at least 2 liters each day. Drinking more water or other liquids is the easiest and most crucial change you can make to your lifestyle to prevent stone illness [51] (Table 5, Ref. [52, 53, 54, 55, 56, 57, 58]).
Table 5: Clinical trial.
| Clinical Trial | Title | Condition | Phase | Treatment | References |
|---|---|---|---|---|---|
| NCT02645058 | RIRS Against ESWL for Treatment of Renal Stones | Kidney Stone | Not Applicable | RIRS (Retrograde intrarenal surgery) | [52] |
| NCT05855057 | Efficacy of US-Guided PCNL surrounding Diverse Positions for Renal Stone Treatment | Kidney Stone | Phase 1 | Flank suspended supine position percutaneous nephrolithotomy | [53] |
| NCT02090439 | Silodosin’s effectiveness when utilised as expulsive therapies for ureteral pelvic stones | Kidney stone | Phase 3 | Drug: Silodosin | [54] |
| NCT02373384 | Predictors of Successful Oral Dissolution Therapy with Radiolucent Renal Stones | Kidney stone | Phase 4 | Drug: Oral alkalinization (Potassium citrate, Allopurinol) | [55] |
| NCT02404701 | Effect of Over-the-counter Dietary Supplements on Kidney Stone Risk | Kidney stone | Not Applicable | Dietary Supplement: Aloe vera with Cranberry | [56] |
| NCT03567421 | Ureteral Stenting Following Ureteroscopy with Stone Treatment options: A Worldwide View on Indications and Results | Kidney Stone | Phase 2 | RIRS (Retrograde intrarenal surgery) | [57] |
| NCT01022060 | Renal Development and Dissolution of Renal Calculi within Patients alongside Recurrent Calcic Lithiasis | Kidney Stone | Phase 3 | Dietary Supplement: Renalo, Placebo | [58] |
ESWL: Extracorporeal Shock Wave Lithotripsy; US: United States; PCNL: Percutaneous nephrolithotomy.
Nutritional aspects of nephrolithiasis
The natural progression of stone diseases among children is less well understood than that in adults [59]. The condition is associated with significant morbidity, including confirmed instances of recurrence fluctuating between 6.5 to 44% [60]. Barring follow-up along with medical intervention, the recurrence probability can approach 50% after 5–6 years. Nephrolithiasis can result in a variety of urine composition concerns.
Urinary abnormalities might be induced by dietary, physiological, or metabolic alterations. Reducing abnormal risk factors through dietary and pharmacological therapies can help avoid repeated stone formation [61]. Urolithiasis epidemiology varies according to location and history.
Vesical stones in children are still a problem in developing countries. Calculi based on ammonium urate as well as calcium oxalate are widely distributed in “primitive” vesical stones across Asia [62]. Malnutrition during childhood is a prominent cause of vesical stones in Turkey, Iran, India, China, Indochina, as well as Indonesia.
However, a decline in prevalence is often observed in conjunction with enhanced socioeconomic conditions.
India, Pakistan, and especially Southern China make up a substantial portion underlying Asia’s stone belt. Calcium oxalate causes 45–65% of all children’s gemstones, followed by calcium phosphate (14–30%), struvite (13%), cystine (5%), uric acid (45%), and lastly mixed as well as miscellaneous Table 6 [63].
Table 6: Dietary factors can influence both oxalate and calcium stone development.
| Dietary factors | Proposed mechanism(s) |
|---|---|
| Oxalate | Excess oxalate excretion in urine |
| Sodium | Increased urinary calcium excretion |
| Animal protein | Calcium and uric acid excretion increased, but citrate extraction was reduced in the urine |
| Vitamin C | Higher oxalate synthesis and excretion |
| Carbohydrates Decreased risk | Increased urinary calcium excretion |
| Dietary calcium Potassium | Urinary citrate excretion rose, whereas calcium excretion declined |
| Phytate | Calcium oxalate absorption and crystallization are inhibited |
| Magnesium | Vitamin B6 deficiency can enhance the development of oxalate and cause oxaluria |
In the 1970s, a high-protein, refined carbohydrate, and salt diet was discovered as a risk factors for oxalate of calcium stones. Nevertheless, the significance of dietary calcium and oxalate remains unknown.
Calcium stone formation may be genetically determined [64].
Although family history is highly associated with idiopathic calcium stone disease, little is known regarding metabolic changes that contribute to this vulnerability and hereditary communication.
Nutrition for children and kidney stones
Idiopathic hypercalciuria in children is commonly treated with dietary or pharmacological measures [65]. The long-term impact of hypercalcemia on broods is unknown. Urinary stones are classified into two types: bladder stones in children (which departed from Europe towards the end nineteenth and early twentieth century), adults with upper urinary tract stones [66].
Improved nutrition has helped to reduce the incidence of endemic bladder stones in various nations along the belt. Stone formation is mostly determined by urine composition, which reflects food trends in the individual countries. A diet low in overall animal protein, calcium, magnesium phosphorus yet rich in acidogenic grains is the leading cause of bladder stones in children [67].
In Thailand, endemic areas have reported early weaning using Pre-masticated rice, veggies, along with undercooked fermented fish as the primary source of animal protein. Vesical stones are more prevalent in places with mild to average protein-energy deficit (PEM) compared to those with severe PEM.
In a retrospective study of 1440 idiopathic stone patients in Pakistan, hypercalciuria was detected in 11%, hyperoxaluria 40%, hyperuricosuria in 27%, and hypocitruria in 63%. Consumption of protein was low in 60 individuals (44%), calcium in 45 (33%), potassium in 105 (77%), alongside oxalate in 75 (55%). The lumps were composed of either calcium oxalate (47%), ammonium hydrogen urate (27%), or struvite (6.4%) [68].
Children without urolithiasis frequently have a lower 24-hour quantity of urine than other children. In the year a study of 32 kids diagnosed with urolithiasis, urine flow greater than 1 mL/kg/h significantly reduced the likelihood of calcium oxalate, calcium phosphate, especially uric acid supersaturation, hence preventing kidney stones.
For a youngster measuring 40 kg, this corresponds to 960 cc of pee every day.
Patients with cystinuria may require higher urine flow, but primary xanthinuria may necessitate significant fluid intake [69]. These people should consume enough milk to satisfy their calcium and protein requirements.
Although excessive fluid consumption has had minimal success in children, it is nevertheless suggested to raise urine volume according to body size. Therapeutic medicines that increase urine citrate concentration may assist children with hypocitraturia. Children with residual stone fragments should be advised to maintain high fluid intake and use potassium citrate to reduce the risk of recurrent stone formation [70].
Nutritional factors for nephrolithiasis
Water and other fluids
According to research, those who consume less than 1.5 L of fluids per day have a 50% higher chance of acquiring kidney stones than those who consume more than 2.5 L.
Two studies, one observational and one interventional, suggest that drinking plenty of water helps prevent kidney disease and lessen recurrence [71]. After a 5-year follow-up, the subsequent recurrence rate decreased by 27% reduced 12% and daily water intake rose from 1 to 2 L.
Although water is essential for avoiding nephrolithiasis, it is unknown if hard water with high divalent ion levels contains the same anti-lithogenic properties as fresh water and leaves little dry residue. Consider trace elements, including calcium, sodium, potassium, chloride, magnesium, iron, fluorine, iodine, zinc, among selenium when determining how much water you consume [72]. However, adopting oligomineral, low NaCl (sodium chloride) water appears to be a viable solution.
Drinks that boost pH, Citric acid along with volume, which includes freshly squeezed oranges with lemons, juices, green tea, and wine, can be a good substitute for water.
Beer prevents calcium stone disease but raises the hazard of urate stone disease due to its high purine-guanosine satisfied [73]. Cranberry juice may not prevent calcium nephrolithiasis, but it can help cure infected stones.
Tea and coffee enhance oxalate levels; however, adding milk can decrease this effect because calcium binds to oxalate and limits absorption. Some drinks, including grapefruit and apple juice, as well as cola, may stimulate lithogenesis through an unknown mechanism [74].
Fluid intake
Low amount of urine, resulting from inadequate one of the most significant risk factors underlying kidney stone formation is excessive fluid consumption as well as loss. Many pharmacological and pathophysiological disorders can cause dehydration, which alters water requirements [75]. These causes include excessive perspiration as a result of temperature exposure, mental stress, and intense workout levels, and profession, as well as persistent diarrhoea as a result of fat malabsorption caused by various gastrointestinal illnesses.
An investigation of 100 steel manufacturing employees discovered that 16% exhibited a history of stone disease, and more exceeding half had urine osmolality levels more than 700 mOsm, suggesting dehydration. Health care workers who have limited access to potable water are furthermore at a higher risk of acquiring stones. A survey of workers revealed that physicians who worked in an operating theatre had the highest occurrence of nephrolithiasis (17.4% compared 9.7%), as well as higher stress levels, in addition to lower fluid consumption compared to workers working elsewhere [76]. Other occupations that can contribute to urolithiasis include professional drivers, aeroplane pilots, and schoolteachers.
Tap and mineral water
The effect of tap versus mineral water concentrations on kidney stone formation is still debated. The composition of drinking water, notably the percentage of divalent cations including magnesium and calcium, varies substantially among geographic regions within the same country.
Hard tap water with a calcium carbonate level of more than 120 mg/L can contribute to the daily consumption of calcium. A study of 2295 individuals from two sites in the United States found that those who consume water from the faucet from a private well are more likely to acquire urinary stones. However, the cause of the higher risk among individual well users remains unknown. Numerous cohort studies demonstrated no relationship between the level of hardness of public water supply and urinary disease associated with stones [77].
Bicarbonate, like calcium, magnesium, and other ions, is a reasonable component of inorganic water, as opposed to tap water. Bicarbonate enhances the body’s buffering capacity and acts as a powerful alkalising agent. Water from minerals rich in bicarbonate might aid in alkalinisation treatment and contribute to urinary inhibitory potential by raising urinary pH affects citrate excretion. Another randomised crossover trial with healthy participants looked at how an equimolar acidic load, either a form of bicarbonate-rich mineral water or potassium citrate, affected the urinary risk profile towards calcium oxalate as well as uric acid stone development.
Consuming 2 L/day of mineral-enriched water with 1715 mg/L bicarbonate, either 2.55 g/day potassium citrate significantly increased urinary pH along with citrate excretion while decreased oxalate excretion [78].
Both categories had a significant reduction in the relative overabundance of calcium oxalate as well as uric acid. A study of healthy persons conducted under controlled dietary conditions discovered that consuming mineral water rich in bicarbonate, calcium, plus magnesium increased urine pH as well as the excretion of citrate and magnesium, which are urinary inhibitors against calcium oxalate stone formation. Calcium excretion rose considerably, although the corresponding supersaturation associated with calcium oxalate remained the same [79].
Fruit juices as well as juice-based drinks
The impact of fruit juices on metabolism is largely influenced by their alkali citrate content. When consumed, dietary citrate is absorbed in the digestive system and transformed into bicarbonate, which can raise both urine pH and the amount of citrate excreted. Citrus juices like lemon, orange, and grapefruit are rich sources of citric acid and can serve as natural alternatives to medicinal alkalizing agents [80]. Among these, orange juice is one of the most commonly consumed worldwide. However, studies on how orange juice affects urine factors linked to kidney stone formation have shown mixed results.
Some large-scale cohort studies suggest that regularly drinking orange juice may lower the risk of developing kidney stones. Controlled trials under specific dietary conditions have shown that orange juice provides an alkaline effect, leading to higher urine pH and citrate output. Still, despite this alkalizing benefit, most studies found that orange juice did not significantly reduce the risk of forming calcium oxalate stones [81]. Although orange juice has a low oxalate content, two out of three studies reported a noticeable rise in urinary oxalate levels, possibly due to the conversion of vitamin C (ascorbic acid) into oxalate inside the body.
Because of concerns about the high sugar and calorie content of orange juice and its low fiber, health experts often recommend eating whole fruits instead. It’s advised to limit fruit juice to one serving a day and to dilute it with water when consumed [82]. In a small crossover trial involving 10 healthy individuals on a regular diet, researchers compared Crystal Light lemonade with two reduced-calorie orange juice drinks. They found that only the Kroger brand low-calorie orange juice had a notable effect, though changes in citrate levels, an important factor in preventing calcium oxalate stones, were not significantly different between the beverages [83].
Additionally, potential health risks from excessive juice consumption and concerns about additives like artificial colors, preservatives, sweeteners, and ingredients such as added ascorbic acid and calcium limit the suitability of these drinks for individuals prone to kidney stones.
Soft drinks
In a large randomized controlled trial involving individuals who regularly consumed soft drinks (at least 160 mL per day), male participants were randomly assigned to either stop drinking soft drinks or continue their usual intake as part of the control group. The results showed that soft drink consumption, especially beverages containing phosphoric acid, was associated with a higher risk of repeated kidney stone formation [84].
Further evidence from large-scale studies, including the Health Professionals Follow-Up Study (HPFS) and Nurses’ Health Studies (NHS I and II), which tracked 194,095 participants over more than eight years, also found a strong link between the intake of sugar-sweetened cola and non-cola soft drinks and an increased risk of kidney stones.
Additionally, a cross-sectional analysis based on the Third National Health and Nutrition Examination Survey (NHANES-III) showed that people who consumed more sugar-sweetened soft drinks had higher levels of uric acid in their blood and were more likely to suffer from hyperuricemia. Long-term cohort studies have further supported this association, identifying a clear connection between sugary soft drink intake and a higher risk of developing gout, particularly in men [85].
One possible explanation for these findings is the high fructose content in sugary soft drinks. Fructose has been shown to raise the risk of kidney stone formation, likely due to its impact on uric acid metabolism and urinary composition.
Tea and coffee
Tea and coffee rank among the most commonly consumed beverages worldwide. According to comprehensive reviews and large population-based studies, regular consumption of tea and coffee may help reduce the risk of kidney stone formation. This protective effect is thought to be largely due to caffeine’s mild diuretic action, which may help offset the calcium loss in urine (hypercalciuria) often linked with stone development [86].
The European Food Safety Authority (EFSA) has deemed a daily caffeine intake of up to 400 mg, roughly the amount in four cups of brewed coffee, as safe for healthy adults, except pregnant women. In addition to caffeine’s diuretic effect, tea might offer further protective benefits by increasing overall fluid consumption and through the antioxidant activity of its natural compounds, such as polyphenols.
However, many of the cohort studies did not distinguish between different types of tea and coffee, such as black, green, herbal, or fruit tea, which limits the precision of their findings. Another concern is the oxalate content present in these beverages. While coffee contains relatively low levels of oxalate, black and green teas vary significantly in oxalate concentration, depending on factors like plant type, harvest timing, and processing methods [87]. Among the teas, black and green varieties tend to have the highest oxalate levels, whereas herbal and fruit teas are typically much lower.
Because of these variations, the exact role and mechanism by which black and green tea may help prevent kidney stones remain unclear and warrant further investigation.
Sodium and calcium chloride
When daily calcium intake increases from 400 mg to 1200 mg, urinary calcium excretion also rises from 120 mg to 180 mg in healthy individuals, and from 240 mg to 400 mg in those with hypercalciuria. Traditionally, people prone to kidney stones have been advised to reduce their intake of milk and dairy products [88]. However, current research does not support this recommendation for several reasons:
1. Cutting down on calcium reduces its binding with oxalate in the gut, which leads to greater oxalate absorption and a higher risk of stone formation.
2. Avoiding dairy may lead patients to increase their consumption of animal protein (such as meat, fish, and poultry), which can negatively affect kidney stone risk.
Studies suggest that consuming around 1000 mg of calcium per day can lower the risk of kidney stones by about 30% compared to those who take in less than 600 mg daily. A five-year randomized clinical trial involving male patients with high urinary calcium showed that a diet with normal calcium intake but reduced salt and animal protein was more effective in preventing stone recurrence than a low-calcium diet [89].
The calcium-excreting effect of table salt is believed to come from its sodium and chloride content, which may impair calcium reabsorption in the kidneys. This, along with the acid load from proteins, can increase the risk of stone formation. Moreover, excess acid and potassium deficiency may reduce urinary citrate levels, a natural inhibitor of kidney stone formation, thereby contributing further to the risk of stone development [90].
Citrate
Citrate plays a key role in preventing the formation of calcium oxalate kidney stones by binding to free calcium ions in the urine. This reduces the saturation of calcium oxalate and prevents crystal formation. A condition known as hypocitraturia or low urinary citrate is commonly observed in people with calcium kidney stones, affecting approximately 19% to 63% of such individuals [91]. As a result, measuring urinary citrate has become a standard part of the metabolic evaluation in stone-forming patients. In many cases, hypocitraturia can be corrected through oral alkali therapy, even though not all tissues respond uniformly to alkali loading.
The most frequent cause of low urinary citrate is metabolic acidosis, which alters how citrate is processed in the kidneys. Under acidic conditions, more citrate converts to its divalent form in the proximal tubules, where it is readily reabsorbed through the Sodium-dependent dicarboxylate transporter 1 (NADC-1) transporter, a protein also found in the small intestine and colon [92]. Research has linked NADC-1 deficiency to an increased risk of kidney stone formation in both human and animal studies. Acidic body conditions tend to lower urinary citrate levels.
A diet low in fruits and vegetables can contribute to hypocitraturia because these foods supply dietary alkali. Their absence leads to a more acidic internal environment, which encourages the kidneys to reabsorb more citrate rather than excrete it. Including more fruits and vegetables in the diet helps increase citrate levels in the urine by lowering hydrogen ion (H⁺) concentration, raising urinary pH, and reducing citrate reabsorption.
For individuals with low citrate levels, a diet rich in fruits and vegetables is recommended. Such a diet not only boosts urinary volume and citrate levels but also provides beneficial alkaline minerals like potassium and magnesium. This dietary approach typically involves reducing animal protein and salt intake as well [93]. Adherence to a DASH (Dietary Approaches to Stop Hypertension) diet significantly increased urinary output, even without increased fluid intake. The high water content and alkaline nature of fruits and vegetables likely account for the observed rise in urine citrate and volume. Multiple studies suggest that the stone-preventing effects of vegetables are due to these beneficial metabolic changes.
Protein
For adults, the recommended protein intake is about 0.8 to 1.0 grams per kilogram of ideal body weight per day. Consuming excessive protein has been linked to changes in urine composition that may raise the risk of kidney stone formation. A high-protein diet increases the body’s acid load, which can lead to higher urinary calcium levels, lower urine pH, and reduced citrate excretion, all of which are known risk factors for stone development [94].
In one study involving 18 patients with hypercalciuria and kidney stones, reducing protein intake to 0.8 g/kg of body weight per day resulted in lower urinary calcium and uric acid levels, along with an increase in urinary citrate excretion. However, systematic reviews have provided mixed results regarding the link between dietary protein and stone risk. For example, a review by Pedersen included two large cohort studies that found no significant association between protein intake and kidney stone development. On the other hand, one well-designed study did report that higher protein intake was associated with increased urinary calcium levels, which could promote calcium stone formation [95].
In healthy individuals, supplementation with 1.5 grams of L-methionine daily had no effect on calcium excretion, but increasing the dose to 3 grams per day resulted in a calcium excretion increase of about 1 mmol per day. So far, no randomized controlled trial has directly compared high versus low protein intake in relation to kidney stone formation risk.
Although the precise relationship between protein consumption and stone risk remains uncertain, large observational studies have shown that a higher dietary acid load, primarily from protein-rich foods, is linked with increased risk of stone formation [96]. Importantly, the balance of protein with alkaline foods like fruits and vegetables may be more predictive of stone risk than protein alone. These plant-based foods help neutralize the acid load from proteins and support higher urine pH and citrate excretion.
In patients with low urinary citrate, adding more fruits and vegetables to the diet has been shown to raise urinary pH, boost citrate levels, and reduce the relative supersaturation of both calcium oxalate and uric acid. Since a highly acidic diet lowers both urinary pH and citrate two important defenses against stone formation, maintaining a diet rich in alkalizing foods is beneficial [97]. Higher urine pH not only promotes the excretion of stone-inhibiting citrate but also enhances calcium binding in the urine, thereby lowering the risk of crystal formation.
Carbohydrates
Research exploring the relationship between carbohydrate intake and kidney stone risk has produced mixed findings. Some studies reported that individuals with kidney stones consumed similar amounts of carbohydrates as healthy controls, while others observed higher carbohydrate intake among stone formers. A major limitation of these studies is their failure to differentiate between types of carbohydrates, especially the common disaccharide sucrose and its components, glucose and fructose [98].
Prospective cohort studies have shown that higher sucrose intake is associated with an increased risk of kidney stone formation in women, though no such link was observed in men. Earlier research revealed that consuming 100 grams of glucose or sucrose increased urinary calcium excretion in both healthy individuals and calcium oxalate stone formers with the latter group showing a more pronounced effect. This rise in urinary calcium was believed to result from enhanced calcium absorption in the intestines and reduced reabsorption in the kidney tubules following a glucose load [99].
It has been suggested that this effect may be partly driven by elevated insulin levels in response to sugar intake. However, a controlled study involving calcium stone patients with idiopathic hypercalciuria and healthy participants on a fixed diet found that high insulin levels (hyperinsulinemia) are unlikely to play a major role in the stone formation process in these patients.
Fructose consumption has increased significantly in recent decades due to its widespread use as a sweetener in processed foods and beverages, often replacing glucose or sucrose [100]. A systematic review and meta-analysis found a positive association between fructose intake and kidney stone risk, although the exact biological mechanisms remain unclear. Fructose may contribute to stone formation by influencing the urinary excretion of calcium, oxalate, and uric acid, altering urine pH, and affecting uric acid metabolism.
Furthermore, a cohort study involving male participants linked higher fructose intake to an increased risk of developing gout, a condition closely tied to elevated uric acid levels [101]. To fully understand how sugars like sucrose, glucose, and fructose affect stone formation, more controlled studies using fixed metabolic diets are needed. Such studies could clarify how these sugars influence urinary chemistry and the risk of forming uric acid or calcium oxalate stones [102].
Fat
The connection between dietary fat intake and the risk of developing kidney stones remains unclear and poorly studied. Some research found no significant difference in fat consumption between individuals with kidney stones and healthy controls, while other studies reported higher fat intake among stone formers.
Emerging evidence suggests that the type of fat consumed, particularly the balance between omega-6 (n-6) and omega-3 (n-3) polyunsaturated fatty acids (PUFAs), may play a role in calcium oxalate stone formation through complex biological pathways [103]. For instance, individuals with idiopathic calcium oxalate stones have been found to have elevated levels of arachidonic acid (C20:4n-6) in their blood plasma and red blood cell membrane phospholipids compared to healthy people.
Arachidonic acid, stored in cell membrane phospholipids, can be released by phospholipase enzymes and converted into prostaglandin E2 (PGE2), a compound linked to increased urinary calcium loss. PGE2 may promote calcium stone formation by enhancing calcium absorption in the intestines, stimulating bone calcium release, and reducing the kidneys’ ability to reabsorb calcium [104]. High levels of arachidonic acid might also contribute to elevated urinary oxalate by enhancing oxalate transport across the intestinal and renal membranes through activation of anion transporters.
In a small study involving 20 healthy participants, supplementation with omega-3 fatty acids, specifically DHA (docosahexaenoic acid, 22:6n-3) and EPA (eicosapentaenoic acid, 20:5n-3) led to their incorporation into cell membrane phospholipids, replacing some of the arachidonic acid content [105]. This dietary shift in fatty acid composition is believed to help reduce the urinary excretion of both calcium and oxalate, potentially lowering the risk of stone formation.
Dietary management
Making changes to the diet is one of the most effective strategies to lower urinary risk factors associated with kidney stone formation, particularly calcium oxalate stones, which are the most common type. However, dietary recommendations should be personalized based on each patient’s specific biochemical and dietary risk profile [106]. Conducting a comprehensive nutritional assessment is an essential part of evaluating patients who form stones and is fundamental to providing effective dietary guidance.
Among the tools available, seven-day dietary records are considered the most reliable for assessing typical eating habits and identifying nutritional patterns linked to stone risk [107]. Multiple dietary factors, such as fluid intake, protein, carbohydrate, oxalate, calcium, and sodium chloride consumption, significantly impact urine composition and influence the likelihood of kidney stone development. Table 7 outlines detailed dietary guidelines tailored for individuals prone to calcium oxalate stones, helping to modify these key dietary elements to reduce stone recurrence and improve overall urinary health [108, 109, 110].
Table 7: Dietary recommendations based on urinary risk factors for calcium oxalate stone formers.
| Urinary Risk Factor | Definition/Limit | Dietary and Lifestyle Recommendations |
|---|---|---|
| Low Urine Volume | Urine output <2.0 L/d | Increase fluid intake to achieve >2.0–2.5 L urine per day. Emphasize neutral or alkalizing fluids (e.g., water, citrus-based beverages). |
| Hypercalciuria | Urinary calcium >5 mmol/d | Maintain daily calcium intake at 1000–1200 mg. Limit sodium chloride and moderate protein intake (0.8–1.0 g/kg body weight/day). Avoid excess salt and animal protein. |
| Hyperoxaluria | Urinary oxalate >0.5 mmol/d | Adopt a low-oxalate diet. Ensure adequate calcium intake (1000–1200 mg/d) to bind oxalate in the gut. Consider calcium supplements with meals in cases of enteric hyperoxaluria. |
| Hyperuricosuria | Urinary uric acid >4 mmol/d | Reduce dietary purines (avoid red meat, organ meats, anchovies, etc.). Moderate protein intake (0.8–1.0 g/kg body weight/day). Increase fruit and vegetable consumption. |
| Hypocitraturia | Urinary citrate <1.7 mmol/d | Increase intake of fruits and vegetables rich in citrate and potassium. Limit animal protein intake (0.8–1.0 g/kg body weight/day). Encourage alkaline-promoting diets (e.g., DASH or Mediterranean). |
DASH: Dietary Approaches to Stop Hypertension.
Preliminary findings on dietary plants in preventing and managing kidney stones
Recent evidence from human studies suggests that a diet rich in fruits and vegetables may play a key role in preventing kidney stone formation, also known as urolithiasis. Large-scale population studies have identified diet as a major contributing factor in kidney health and disease risk [111]. Smaller clinical trials indicate that diets emphasizing plant-based proteins rather than those derived from animals can help reduce the body’s acid levels, slow down kidney damage in people with chronic kidney disease, and improve glomerular filtration rate (GFR). These plant-based dietary approaches, especially when combined with sodium-based alkali supplements, are considered important preventive strategies for individuals with reduced kidney function [112].
Regular consumption of a plant-based diet has been shown to raise urine pH and increase urine output. It also boosts the levels of natural stone-preventing substances in the urine, such as citrate, phytate, potassium, and magnesium. These components help to reduce the supersaturation of calcium oxalate and uric acid, which are the primary compounds involved in kidney stone formation. Phytate a naturally occurring form of phosphate in plant foods has been found to bind with calcium in the digestive tract, lowering the chances of crystal formation in the urine and thus reducing stone risk. Moreover, plant-derived alkaline compounds enhance urinary citrate levels, a known inhibitor of stone development [113].
In addition, dietary fiber abundant in fruits and vegetables may further support kidney stone prevention. Fiber binds with minerals and fats in the intestines, which can reduce the amount of oxalate and calcium that enters the urine. A study examining the dietary habits of women found that those who consumed more plant-based foods, fruits, and vegetables were less likely to have a history of kidney stones [114]. Even among women who had previously experienced stones, increased intake of these foods was associated with a lower risk of recurrence.
Role of dietary plants in preventing kidney stones
Using dietary strategies is considered an effective and practical approach to protect kidney health. These interventions can work alone or alongside genetic and lifestyle factors to help prevent kidney stones. Plant-based nutrition, in particular, has shown promise in reducing the recurrence of calcium oxalate stones, the most common type of kidney stones [115].
In the following section, we explore a variety of dietary plants, natural food additives, fruits, and vegetables that have demonstrated protective effects against kidney stone formation. Each of these natural agents offers specific benefits that contribute to the prevention of urolithiasis, supported by experimental and clinical evidence.
Green tea
Green tea (Camellia sinensis) has been widely used as a traditional remedy due to its rich content of polyphenols, which give it strong antioxidant properties. Although green tea naturally contains oxalates and may not be ideal for individuals prone to calcium oxalate kidney stones, it has still attracted considerable interest as a dietary supplement for those with kidney stone issues. This is because of its potential anti-stone (antilithogenic), heart-protective (anti-atherosclerotic), and antioxidant effects [116].
Key compounds in green tea, known as catechins such as epigallocatechin gallate (EGCG), epicatechin gallate (ECG), epigallocatechin (EGC), and epicatechin (EC), have been found to guard the kidneys against oxalate damage. Experimental studies in rats showed that green tea intake reduced the supersaturation of brushite (a type of calcium phosphate), lowered the expression of osteopontin (OPN) and superoxide dismutase (SOD), improved the Bcl-2 protein levels, and reduced kidney cell death (apoptosis) [117].
Overall, these findings suggest that green tea, because of its antioxidant components, may help lower the formation of calcium-based kidney stones.
Raspberry
Raspberry (Rubus idaeus), a fruit from the Rosaceae family, is widely cultivated in parts of Europe and the Mediterranean region and has long been valued for its nutritional and medicinal benefits. Recent studies suggest that raspberries may help reduce the risk of kidney stones, even after short-term use [118].
Research has shown that raspberries are particularly effective against calcium oxalate stones the most common type of kidney stone. In animal studies, the aqueous extract of raspberry significantly reduced the buildup and crystallization of calcium oxalate in the kidneys. It also helped break down existing crystal matrices. Rats treated with raspberry extract showed lower levels of harmful markers such as malondialdehyde (MDA) and protein carbonyls, as well as decreased urinary calcium and phosphorus levels [119].
These findings suggest that raspberries may offer protective benefits against kidney stone formation through their antioxidant and crystal-inhibiting effects.
Rubia cordifolia
Rubia cordifolia, commonly known as madder or Indian madder, belongs to the Rubiaceae (coffee) family and has traditionally been used as a natural dye in foods. Phytochemical studies of R. cordifolia have shown that it contains several beneficial compounds, such as glycosides, triterpenoids, anthraquinones, saponins, quinones, and tannins. These bioactive components have made the plant useful in managing a wide range of health conditions, including jaundice, diabetic foot ulcers, and cardiovascular problems [120].
In addition to these benefits, R. cordifolia has shown potential in supporting kidney health and preventing the formation of urinary stones. Its extract helps reduce the development and accumulation of calcium oxalate crystals in the kidneys. This effect may be due to its ability to restore magnesium levels, reduce protein loss in urine (proteinuria), and lower uric acid excretion [121]. Its antioxidant properties likely contribute to its overall kidney-protective (nephroprotective) action.
Parsley
Parsley (Petroselinum crispum), a versatile plant from the Umbelliferae family, is commonly used as an herb, spice, and vegetable across Western Asia, the Mediterranean, and Europe. Research has highlighted its numerous health benefits, including antioxidant, anti-inflammatory, diuretic, kidney-protective (nephroprotective), enzyme-regulating, and blood pressure-lowering effects [122]. These properties are largely attributed to its rich content of bioactive compounds such as flavonoids, carotenoids, coumarins, tocopherol (vitamin E), and ascorbic acid (vitamin C).
Parsley has also been recognized for its potential to help prevent kidney stones. In animal models of calcium oxalate stone formation, parsley extract significantly reduced the formation of calcium oxalate crystals, decreased urine supersaturation, and lowered protein excretion in urine [123]. Its high content of chlorophyll and magnesium is thought to reduce the risk of stone development by preventing oxalate overload and dehydration of crystals. Additionally, parsley helps maintain an optimal urine pH, which keeps calcium oxalate particles dispersed and easier to eliminate from the urinary system.
Pomegranate (punica granatum)
Pomegranate (Punica granatum) has a long history of use in traditional medicine and is often referred to as “a pharmacy in itself” due to its wide range of therapeutic compounds. The fruit is rich in powerful antioxidants such as polyphenols, anthocyanins, and alkaloids, which help neutralize harmful free radicals [124]. Almost every part of the plant, including its seeds, juice, peel, flowers, and seed oil, has been used for both preventive and therapeutic purposes.
In traditional practices, pomegranate seeds are used to ease urinary discomfort and burning sensations. Its juice and extracts have been employed to protect the kidneys from toxic damage, while the peel and flowers have shown potential in treating kidney dysfunction and supporting renal artery health. One of the most notable benefits of pomegranate is its ability to reduce excessive calcium levels in urine (anti-hypercalciuria) and prevent the formation of kidney stones (anti-urolithiasis), making it a valuable natural agent in the prevention of renal stone formation.
Ammi visnaga
Ammi visnaga has been used for centuries in Egyptian traditional medicine, particularly in the form of herbal teas made from its fruits, to treat kidney stones. Research has shown that an aqueous extract from this plant can help speed up the breakdown of cystine stones.
Two of its primary active compounds, khellin and visnagin, have demonstrated beneficial effects in managing kidney stone formation caused by hyperoxaluria in experimental models. In male rats, these compounds helped reduce the build-up of calcium oxalate crystals, increased the excretion of citrate (a natural inhibitor of stone formation), and lowered the amount of oxalate excreted in urine [125]. These findings highlight Ammi visnaga as a promising natural approach to preventing and treating certain types of kidney stones.
Nigella sativa
Nigella sativa, commonly known as black seed, has been widely used in Iranian traditional medicine to help treat urinary stones. Scientific studies using ethylene glycol-induced kidney stone models in rats have shown that ethanolic extracts of Nigella sativa seeds significantly reduced the formation of calcium oxalate deposits in both the kidneys and the urine.
The herb’s main active compound, thymoquinone, displayed both preventive (prophylactic) and treatment (therapeutic) properties against kidney stone formation. In animal studies, thymoquinone effectively decreased the size and number of calcium oxalate crystals within the renal tubules, demonstrating its potential as a natural remedy for managing and preventing kidney calculi [126].
Hibiscus sabdariffa
Hibiscus sabdariffa, widely recognized in traditional Thai medicine, has long been used for both the treatment and prevention of urinary stones. This medicinal plant is rich in active compounds, including polyphenols, anthocyanins, vitamin C (L-ascorbic acid), quercetin, and protocatechuic acid.
Experimental studies have demonstrated that aqueous extracts of Hibiscus sabdariffa exhibit strong antiurolithiatic effects. In animal models where kidney stones were induced using ethylene glycol, the extract significantly reduced the accumulation of stone-forming substances in the kidneys and blood serum [127]. Additionally, in rats fed a glycolate-enriched diet, the extract helped reduce oxalate retention time in the kidneys and promoted its excretion through urine, showing clear potential in limiting stone formation.
Origanum vulgare
Origanum vulgare, commonly known as oregano, has been traditionally used as a lithotriptic (stone-dissolving agent), diuretic, antispasmodic, and culinary spice. Scientific studies have shown that a crude aqueous-methanolic extract of the aerial parts of this plant can inhibit the formation and clustering of calcium oxalate crystals in laboratory (in vitro) settings, significantly reducing crystal development in calcium oxalate supersaturated solutions [128].
Animal studies using ethylene glycol and ammonium chloride to induce kidney stones demonstrated that this extract exerted a strong antiurolithic effect, likely by preventing crystal growth, protecting kidney cells, and offering antioxidant and antispasmodic properties [129]. These protective actions are believed to stem from the plant’s diverse bioactive compounds, including flavonoids, terpenes, coumarins, saponins, alkaloids, sterols, and tannins.
Strategies to prevent kidney stones (urolithiasis)
Preventing kidney stones starts with identifying and addressing their root causes. Whether someone is trying to prevent their first stone or avoid a recurrence, dietary adjustments and proper medication use are essential. Since these approaches are affordable and widely applicable, they offer significant public health benefits. Among all strategies, dietary changes are the most effective in preventing kidney stones.
One of the most important lifestyle changes is to increase fluid intake, ensuring that urine output stays above 2 liters per day. More water helps dilute stone-forming substances like calcium oxalate and reduces the concentration of these crystals in the urine [130].
Dietary recommendations must be tailored to each individual based on their metabolic risk factors. For example, in people with absorptive hyperoxaluria, reducing foods high in oxalate while maintaining adequate dietary calcium can help. Calcium binds to oxalate in the gut, reducing its absorption and risk of stone formation.
A high-salt diet can raise calcium levels in urine by interfering with calcium reabsorption in the kidneys, so it’s wise to cut back on sodium. Similarly, animal protein (such as meat, fish, and poultry), which contains sulfur-rich amino acids, can increase the acid load in the body. This may result in lower urine pH and reduced citrate levels, both of which contribute to stone formation.
If the urine becomes too acidic, limiting animal protein and vitamin D-rich foods may help, while increasing the intake of potassium-rich fruits and vegetables can restore balance.
It’s also important to note that cutting calcium too much can backfire. Low calcium intake may increase the body’s absorption of dietary oxalate, leading to more oxalate in the urine and a higher risk of stones. Calcium supplements, when taken with meals, may help by binding oxalate in the gut. However, the benefits of calcium supplements remain uncertain.
In addition, excessive vitamin C (ascorbic acid) can be converted into oxalate in the body, so its intake should be kept in check [131].
To prevent stones like calcium oxalate, uric acid, and cystine, the goal is to alkalize the urine using fruits, vegetables, citrate supplements, or alkaline mineral water. For those prone to uric acid stones, managing gout is vital, and for cystine stones, limiting salt and protein is recommended.
In contrast, acidic urine helps prevent calcium phosphate and struvite stones. For struvite stones, acidifying urine is a key treatment strategy. Regular follow-up care is essential to confirm that infections are cleared, as infections can contribute to stone formation.
Unfortunately, current medications are often insufficient to fully prevent kidney stones, which highlights the need for further research and new therapeutic options [132].
Urological interventions in kidney stone management
Surgical intervention becomes necessary when medical treatments fail or emergency decompression is required [133, 134, 135, 136, 137, 138, 139]. However, there is no universally accepted timeline for when to proceed with surgical procedures [140, 141, 142, 143, 144, 145] (see Table 8). The three primary treatment options include Extracorporeal Shock Wave Lithotripsy (ESWL), Ureteroscopy (URS), and Percutaneous Nephrolithotomy (PCNL). The choice of procedure depends on factors like stone size, location, the surgeon’s expertise, and the availability of specialized equipment.
Table 8: Comparative overview of therapeutic modalities for renal and ureteral stone management.
| Treatment Modality | Indication | Stone-Free Rate (%) | Limitations | Complications |
|---|---|---|---|---|
| Shock Wave Lithotripsy (SWL) | Small renal and ureteral stones | 80–83 | No direct visualization; high retreatment rate | Steinstrasse, perirenal hemorrhage |
| Ureteroscopy (URS) | Small-to-medium renal and ureteral stones | 85–88 | Requires adult-sized equipment; operator-dependent technique | Ureteral perforation, infection, strictures, hematuria |
| Percutaneous Nephrolithotomy (PCNL) | Large/complex renal calculi (>2 cm), staghorn stones | 70–97 | Invasive; requires general anesthesia, surgical expertise, and hospitalization | Bleeding (8–16% transfusion), urinary leakage, fever, sepsis |
| Mini-PCNL/Ultra-Mini PCNL | Medium-sized renal stones (1–2 cm) | 82–95 | Narrow working channel; limited in large stone burden | Similar to PCNL but lower bleeding risk |
| Open Pyelolithotomy | Very large or multiple complex stones | 79–98 | Highly invasive; longer hospital stay and recovery time | Risks of open surgery: infection, scarring, delayed recovery |
| Minimally Invasive Pyelolithotomy | Large renal stones (in selected cases) | Not well documented | Learning curve; limited literature | Similar to other minimally invasive procedures |
| Laparoscopic Pyelolithotomy | Large solitary stones not amenable to SWL/URS | 85–95 | Technically demanding; requires advanced laparoscopic skills | Injury to adjacent structures, prolonged anesthesia |
| Robotic-Assisted Stone Removal | Large impacted stones with anatomical challenges | ~90 | High cost, limited availability in low-resource settings | Same as laparoscopic; reduced tactile feedback |
| Medical Expulsive Therapy (MET) | Small distal ureteric stones (<10 mm) | 35–65 | Limited to select cases; slower response | Delayed stone passage may lead to obstruction or infection |
| Anatrophic Nephrolithotomy | Complex staghorn calculi in non-functioning kidneys | 70–90 | Major surgery; risk of renal ischemia | Hemorrhage, renal impairment, infection |
ESWL (extracorporeal shock wave lithotripsy)
ESWL is often preferred for treating small stones in the upper urinary tract, especially in children, because it is non-invasive, relatively simple, and effective. In the short term, the stone-free rate ranges from 57% to 97%, and in the long term, between 57% and 92%. ESWL works best for stones less than 20 mm located in the renal pelvis or calyces. Its effectiveness is lower for larger stones or those located in the distal ureters [134].
Possible short-term side effects include blood in urine (haematuria), pain, fever, stone fragments blocking the ureter (steinstrasse), and small internal bleeds (hematomas), although these are generally rare.
The long-term safety of ESWL in children remains unclear. Most studies show no lasting damage to kidney structure or function in children, but these studies are often limited by small participant numbers and short observation periods. Some recent data suggests a potential link to high blood pressure following ESWL, but further research is needed to fully understand this risk [135].
URS (ureteroscopy)
URS is another safe and effective method for treating kidney stones in infants and young patients, particularly for stones ≤20 mm in the mid or lower ureter. A systematic review of over 1700 procedures showed an average stone-free rate of 87.5%, with a 10.5% complication rate, mostly of mild to moderate severity (Clavien Grade I–III) [136].
However, for children under six, URS may require pre-stenting (inserting a tube before the procedure) due to the increased risk of complications or failure in younger patients.
PCNL (percutaneous nephrolithotomy)
PCNL is typically reserved for large stones, complex cases, blockages due to stones, or when other treatments do not succeed. It is especially useful for patients with high stone burden or persistent kidney infections caused by stones [137].
PCNL has a high success rate (around 90%), but it also carries more significant risks, such as bleeding requiring transfusion, injury to surrounding organs, and infection [138].
To reduce these risks, newer, minimally invasive forms of PCNL have been developed, such as mini-PCNL, ultramini-PCNL, and micro-PCNL. These techniques use smaller instruments, which help lower the chance of complications while still maintaining effective stone removal [139].
Impact of vegetarian and vegan diets on kidney stone formation and recurrence
According to the Vegetarian Society, a vegetarian diet avoids all products that involve the killing of animals, such as meat, poultry, fish, and seafood [146]. However, many vegetarians still include dairy and eggs in their meals (lacto-ovo vegetarians), while others ovo-vegetarians exclude dairy but continue to eat eggs. In contrast, vegans follow a much stricter regimen, eliminating all animal-based foods, including dairy and eggs [147].
A review of dietary influences on kidney stone formation suggests that the most effective strategy for reducing stone risk involves eating a diet rich in fruits and vegetables, limiting animal proteins, moderate low-fat dairy intake, and low salt consumption [148]. These recommendations closely resemble a balanced vegetarian diet that still includes dairy products. In comparison, vegan diets while plant-based tend to be higher in oxalates and lower in calcium due to the exclusion of dairy, which may increase the risk of calcium oxalate stone formation [149].
Vegetarians generally consume a similar amount of calcium as the general population, but vegans tend to consume less calcium, potentially increasing stone risk. So far, no major studies have directly compared the risk of kidney stones in vegan versus vegetarian populations [150]. However, Robertson hypothesized that a vegetarian lifestyle could lead to a 40% to 60% lower chance of developing stones compared to non-vegetarians, even when adjusting for age, gender, and socioeconomic differences.
In a large study from the Oxford cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC), researchers examined how different diets ranging from high meat intake to vegetarianism affected kidney stone risk. Among over 51,000 participants, 303 new kidney stone cases were recorded during more than 716,000 person-years of follow-up [151]. Compared to those who ate large amounts of meat, vegetarians and people with low meat intake had significantly lower risks of kidney stones, with hazard ratios of 0.69 and 0.52, respectively. Interestingly, red meat and poultry were more strongly linked to stone formation than processed meats, and higher fruit consumption was linked to a lower risk [152].
These results align with findings from studies on the DASH (Dietary Approaches to Stop Hypertension) and Mediterranean diets, which both emphasize plant-based foods. In a U.S. cohort of over 241,000 men and women, researchers tracked adherence to the DASH diet for up to 18 years. The diet was scored based on intake of fruits, vegetables, nuts, low-fat dairy, whole grains, and low consumption of salt, sugary drinks, and red meat [153, 154]. Those with the highest DASH scores had significantly lower risks of developing stones, with relative risks of 0.55, 0.58, and 0.60 in men, older women, and younger women, respectively, compared to typical American diets [155].
The Mediterranean diet, which focuses on plant-based foods and uses less red meat, showed similar protective benefits. In a study of 16,094 participants with no prior history of kidney stones, those who most closely followed the Mediterranean diet had hazard ratios of 0.93 and 0.64 for developing stones, compared to less adherent individuals [156]. However, people consuming more monounsaturated fats compared to saturated fats were unexpectedly found to have a higher stone risk than those who ate more vegetables and dairy products.
Because individuals with kidney stones also face higher risks of heart disease and kidney failure, following the Mediterranean diet offers added benefits. Research shows that this eating pattern helps reduce both risks [157].
Interestingly, a case-control study from China with over 2000 participants found that certain vegetarian-style diets might increase stone risk, particularly among women. Higher intake of grains and beans was associated with a greater chance of kidney stone development. Consuming more than three servings of green vegetables daily was also linked to increased stone risk in both men and women [158, 159].
The role of dietary fiber in stone prevention remains controversial. Some evidence suggests that high-fiber, low-calcium diets may reduce urinary calcium but also raise oxalate levels, potentially increasing calcium oxalate saturation in urine [160]. Other studies, such as the EPIC-Oxford cohort, found that fiber might be helpful in reducing stone risk, but vegetable intake by itself was neither beneficial nor harmful [161, 162].
Conclusion
Kidney stones, or renal calculi, are hard mineral deposits that form inside the kidneys and pose a major health challenge worldwide, impacting around 12% of people globally. Their development is influenced by both environmental conditions and metabolic disorders. Among the various types, calcium oxalate and calcium phosphate stones are the most common, making up about 70% of all cases, especially in economically advanced countries. Fortunately, preventive measures such as staying well-hydrated and making specific dietary changes have been shown to effectively reduce the chances of forming these painful stones.
Pharmacological interventions such as Thiazides, Allopurinol, Potassium Alkali, and Tiopronin have demonstrated clinical efficacy in reducing stone recurrence through mechanisms that regulate urinary excretion of minerals. In addition, non-pharmacological treatments utilizing herbal remedies like Virataradigana, Crateava nurvala, and Boerhaavia diffusa have shown potential in alleviating symptoms and preventing stone aggregation through their diuretic and antiurolithiatic properties.
While current evidence supports the therapeutic effectiveness of these interventions, further clinical trials are crucial to expanding understanding of both pharmacological and herbal treatments. Such studies would not only validate traditional approaches but also contribute to enhanced management strategies for nephrolithiasis. Thus, a comprehensive integration of conventional medicine and herbal therapeutics could pave the way for improved patient outcomes and reduced incidence of kidney stone recurrence.
Abbreviations
CaOx, calcium oxalate; CaP, calcium phosphate; CAP, calcium phosphate stones; DASH, Dietary Approaches to Stop Hypertension; EC, epicatechin; ECG, epicatechin gallate; EGCG, epigallocatechin gallate; ESWL, extracorporeal shock wave lithotripsy; GFR, glomerular filtration rate; MDA, malondialdehyde; OPN, osteopontin; PCNL, percutaneous nephrolithotomy; PGE2, prostaglandin E2; PEM, protein-energy malnutrition; RIRS, retrograde intrarenal surgery; NaCl, sodium chloride; NADC-1, sodium dicarboxylate cotransporter 1; SOD, superoxide dismutase; UTI, urinary tract infection; E. coli, Escherichia coli; UTIs, urinary tract infections; HPFS, Health Professionals Follow-Up Study; NHS, Nurses’ Health Studies; NHANES, National Health and Nutrition Examination Survey; PUFAs, polyunsaturated fatty acids; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; EGC, epigallocatechin; URS, Ureteroscopy; EPIC, European Prospective Investigation into Cancer and Nutrition; EFSA, European Food Safety Authority.
Availability of data and materials
The data and supporting information are available within the article.
Author contributions
PS and AP—designed the research study; wrote the manuscript. PS—performed the research and collected the data. AP—analyzed and interpreted the results. Both authors contributed to editorial changes in the manuscript. Both authors read and approved the final manuscript.
Ethics approval and consent to participate
The authors did not conduct any research on humans or animals for this paper.
Acknowledgment
The authors gratefully acknowledge the support provided by Sanskriti College of Higher Education and Studies, Kanpur Dehat, Uttar Pradesh (UP) for facilitating this study. The institution offered administrative assistance and academic infrastructure that contributed to the successful completion of this work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare no conflict of interest.
REFERENCES
1. Danilovic A, Marchini GS, Pucci ND, Coimbra B, Torricelli FC, Batagello C, et al. Effect of a low-calorie diet on 24-hour urinary parameters of obese adults with idiopathic calcium oxalate kidney stones. International Brazilian Journal of Urology. 2021; 47: 1136–1147.
2. Wu ZB, Jiang T, Lin GB, Wang YX, Zhou Y, Chen ZQ, et al. Tea consumption is associated with increased risk of kidney stones in Northern Chinese: a cross-sectional study. Biomedical and Environmental Sciences. 2017; 30: 922–926.
3. Akarken I, Tarhan H, Ekin RG, Çakmak Ö, Koç G, İlbey YÖ, et al. Visceral obesity: a new risk factor for stone disease. Canadian Urological Association Journal. 2015; 9: E795.
4. Astolfi RH, Carrera R, Gattas N, Bertolla R, Sepulveda F, Reggio E, et al. Current scenario of endourological treatment of kidney stones in brazil: results of a national survey. International Brazilian Journal of Urology. 2020; 46: 400–408.
5. Singh P, Enders FT, Vaughan LE, Bergstralh EJ, Knoedler JJ, Krambeck AE, et al. Stone composition among first-time symptomatic kidney stone formers in the community. Mayo Clinic Proceedings. 2015; 90: 1356–1365.
6. Ferraro PM, Curhan GC. Long-term Adverse outcomes of urolithiasis. American Journal of Kidney Diseases. 2018; 72: 774–775.
7. Sikarwar V. Herbal remedies for kidney stone. Contemporary Advances in Science & Technology. 2022; 5: 135–142.
8. Alelign T, Petros B. Kidney stone disease: an update on current concepts. Advances in Urology. 2018; 2018: 3068365.
9. Qaseem A, Dallas P, Forciea MA, Starkey M, Denberg TD; Clinical Guidelines Committee of the American College of Physicians. Dietary and pharmacologic management to prevent recurrent nephrolithiasis in adults: a clinical practice guideline from the American College of Physicians. Annals of Internal Medicine. 2014; 161: 659–667.
10. Daudon M, Frochot V, Bazin D, Jungers P. Drug-induced kidney stones and crystalline nephropathy: pathophysiology, prevention and treatment. Drugs. 2018; 78: 163–201.
11. Abbas W, Akram M, Sharif A. Nephrolithiasis; prevalence, risk factors and therapeutic strategies: a review. Madridge Journal of Internal and Emergency Medicine. 2019; 3: 90–95.
12. Gambaro G, Croppi E, Coe F, Lingeman J, Moe O, Worcester E, et al. Metabolic diagnosis and medical prevention of calcium nephrolithiasis and its systemic manifestations: a consensus statement. Journal of Nephrology. 2016; 29: 715–734.
13. Ma Q, Fang L, Su R, Ma L, Xie G, Cheng Y. Uric acid stones, clinical manifestations and therapeutic considerations. Postgraduate Medical Journal. 2018; 94: 458–462.
14. Moe OW, Abate N, Sakhaee K. Pathophysiology of uric acid nephrolithiasis. Endocrinology and Metabolism Clinics. 2002; 31: 895–914.
15. Gambaro G, Trinchieri A. Recent advances in managing and understanding nephrolithiasis/nephrocalcinosis. F1000Research. 2016; 5: F1000 Faculty Rev-695.
16. Sohgaura A, Bigoniya P. A review on epidemiology and etiology of renal stone. American Journal of Drug Discovery and Development. 2017; 7: 54–62.
17. Eisner BH, Goldfarb DS, Pareek G. Pharmacologic treatment of kidney stone disease. Urologic Clinics. 2013; 40: 21–30.
18. Evan AP, Worcester EM, Coe FL, Williams J, Lingeman JE. Mechanisms of human kidney stone formation. Urolithiasis. 2015; 43: 19–32.
19. Mittal A, Tandon S, Singla SK, Tandon C. In vitro inhibition of calcium oxalate crystallization and crystal adherence to renal tubular epithelial cells by Terminalia arjuna. Urolithiasis. 2016; 44: 117–125.
20. Siener R. Nutrition and kidney stone disease. Nutrients. 2021; 13: 1917.
21. Alanazi NF, Alanazi MA, Alanazi BA, Alsaleh AK, Alomayri MI, Alanazi AT, et al. Renal colic disease: overview, management, and prevention. Journal of Biochemical Technology. 2020; 11: 85–88.
22. Dursun M, Otunctemur A, Ozbek E. Kidney stones and ceftriaxone. EMJ Urology. 2015; 3: 68–74.
23. Naik RV, Patil SB. A review on pathogenesis, diagnosis, and management of urolithiasis. Journal of Pharma Insights and Research. 2025; 3: 075–085.
24. Anlauf M, Hein L, Hense HW, Köbberling J, Lasek R, Leidl R, et al. Complementary and alternative drug therapy versus science-oriented medicine. German Medical Science. 2015; 13: Doc05.
25. Ebert N, Bevc S, Bökenkamp A, Gaillard F, Hornum M, Jager KJ, et al. Assessment of kidney function: clinical indications for measured GFR. Clinical Kidney Journal. 2021; 14: 1861–1870.
26. Stepanova N. Balancing stone prevention and kidney function: a therapeutic dilemma. Journal of Clinical Medicne. 2025; 14: 3678.
27. Ibis F, Yu TW, Penha FM, Ganguly D, Nuhu MA, Van Der Heijden AE, et al. Nucleation kinetics of calcium oxalate monohydrate as a function of pH, magnesium, and osteopontin concentration quantified with droplet microfluidics. Biomicrofluidics. 2021; 15: 064103.
28. Sobirov I, Erniyozov B, Aliqulov J. Urolithiasis pathogenesis risk factors and modern treatment approaches. Frontiers of Global Science. 2025; 3: 53–58.
29. Sun XY, Chen JY, Rao CY, Ouyang JM. Size-dependent cytotoxicity of hydroxyapatite crystals on renal epithelial cells. International Journal of Nanomedicine. 2020; 15: 5043–5060.
30. Kulsoom, Ahmad S, Urwa, Khan IA, Awais, Pricope R, et al. Associations between clinical, biochemical, and nutritional factors in kidney stone formation and recurrence. Urolithiasis. 2025; 53: 112.
31. Saifullah F, Saeed MA. Kidney stones: pathophysiology, cutting-edge treatments, and emerging concerns. Currents in Pharmaceutical Research. 2025; 2: 89–118.
32. Shafi H, Moazzami B, Pourghasem M, Kasaeian A. An overview of treatment options for urinary stones. Caspian Journal of Internal Medicine. 2016; 7: 1–6.
33. Damian DJ, McNamee R, Carr M. Changes in selected metabolic parameters in patients over 65 receiving hydrochlorothiazide plus amiloride, atenolol or placebo in the MRC elderly trial. BMC Cardiovascular Disorders. 2016; 16: 1–9.
34. Huang R, Zhang YH, Huang H, Yang HS. The oxalate content of oolong tea and its relationship with soaking times. Urolithiasis. 2016; 44: 477–478.
35. Hoppe B, Niaudet P, Salomon R, Harambat J, Hulton SA, Van’t Hoff W, et al. A randomised Phase I/II trial to evaluate the efficacy and safety of orally administered Oxalobacter formigenes to treat primary hyperoxaluria. Pediatric Nephrology. 2017; 32: 781–790.
36. Sakhaee K. Medical measures for secondary prevention of urolithiasis. European Urology Focus. 2017; 3: 10–12.
37. Morgan MS, Pearle MS. Medical management of renal stones. The BMJ. 2016; 352: i52.
38. Malihi Z, Wu Z, Stewart AW, Lawes CM, Scragg R. Hypercalcemia, hypercalciuria, and kidney stones in long-term studies of vitamin D supplementation: a systematic review and meta-analysis. The American Journal of Clinical Nutrition. 2016; 104: 1039–1051.
39. Ceylan K, Topal C, Erkoc R, Sayarlioglu H, Can S, Yilmaz Y, et al. Effect of indapamide on urinary calcium excretion in patients with and without urinary stone disease. Annals of Pharmacotherapy. 2005; 39: 1034–1038.
40. Tavasoli S, Alebouyeh M, Naji M, Shakiba majd G, Shabani Nashtaei M, Broumandnia N, et al. Association of intestinal oxalate‐degrading bacteria with recurrent calcium kidney stone formation and hyperoxaluria: a case-control study. BJU International. 2020; 125: 133–143.
41. Spivacow FR, Del Valle EE, Lores E, Rey PG. Kidney stones: composition, frequency and relation to metabolic diagnosis. Medicina. 2016; 76: 343–348.
42. Astroza GM, Neisius A, Tsivian M, Preminger GM, Lipkin ME. Treatment response in patients with stones, and low urinary pH and hypocitraturia stratified by body mass index. The Journal of Urology. 2016; 195: 653–657.
43. Rizwan B. Health benefits of asparagus. Pakistan Journal of Health Sciences. 2020; 1: 14–16.
44. Khan F, Haider MF, Singh MK, Sharma P, Kumar T, Neda EN. A comprehensive review on kidney stones, its diagnosis and treatment with allopathic and ayurvedic medicines. Urology & Nephrology Open Access Journal. 2019; 7: 69–74.
45. Sachdeva S, Kaur J, Mehta S, Saharan R, Nain P. Formulation of ayurvedic medicines and extracts of medicinal plants as an alternative therapeutic treatment option for nephrolithiasis. World Journal of Traditional Chinese Medicine. 2023; 9: 278–283.
46. Azam F, Munier S, Batoo M, Ahmad B, Abbas G. A review on advancements in ethnomedicine and phytochemistry of Tribulus terrestris—a plant with multiple health benefits. International Journal of Biosciences. 2019; 14: 21–37.
47. Narendra K, Swathi J, Sowjanya KM, Satya AK. Phyllanthus niruri: a review on its ethno botanical, phytochemical and pharmacological profile. Journal of Pharmacy Research. 2012; 5: 4681–4691.
48. Niu Z, Duan Z, He W, Chen T, Tang H, Du S, et al. Kidney function decline mediates the adverse effects of per- and poly-fluoroalkyl substances (PFAS) on uric acid levels and hyperuricemia risk. Journal of Hazardous Materials. 2024; 471: 134312.
49. Tolsarwad GS, Biradar MM, Shinde SA. Potential pharmacognostic interventions of Crataeva nurvala: a pharmacological views. Innovations in Pharmaceuticals and Pharmacotherapy. 2020; 8: 66–73.
50. Wang X, Wang Q. Current dietary and medical prevention of renal calcium oxalate stones. International Journal of General Medicine. 2024; 17: 1635–1649.
51. Santarosa BP, Ferreira DO, Surian SR, Tremori TM, Hooper HB, Silva PD, et al. Clinical and anatomopathological study of urolithiasis in feedlot lambs subjected to diets with different phosphorus concentrations. Ciência Animal Brasileira. 2021; 22: e67849.
52. Sharma S, Sharma N, Gupta PC, Verma R, Yadav V. An update on kidney stones: types, mechanism and treatment approaches. Research Journal of Pharmacognosy and Phytochemistry. 2023; 15: 53–62.
53. Abdulrida JJ, Kadhim HY. Assessment of patient’s knowledge about avoidance of recurrent urolithiasis. Kufa Journal for Nursing Sciences. 2015; 5: 1–9.
54. Knight J, Nigam Y, Jones A. Effects of bedrest 4: renal, reproductive and immune systems. Nursing Times. 2019; 115: 51–54.
55. Bosio A, Alessandria E, Dalmasso E, Agosti S, Vitiello F, Vercelli E, et al. Flexible ureterorenoscopy versus shockwave lithotripsy for kidney stones ≤2 cm: a randomized controlled trial. European Urology Focus. 2022; 8: 1816–1822.
56. El-Shaer W, Abdel-Lateef S, Torky A, Elshaer A. Complete ultrasound-guided percutaneous nephrolithotomy in prone and supine positions: a randomized controlled study. Urology. 2019; 128: 31–37.
57. Ding H, Ning Z, Dai Y, Shang P, Yang L. The role of Silodosin as a new medical expulsive therapy for ureteral stones: a meta-analysis. Renal Failure. 2016; 38: 1311–1319.
58. Elbaset MA, Taha DE, Anas M, Abouelkheir RT, Edwan M, Abdullateef M, et al. Optimization of shockwave lithotripsy use for single medium sized hard renal stone with stone density ≥1000 HU. A prospective study. World Journal of Urology. 2022; 40: 243–250.
59. Canvasser NE, Rivera M, Bechis SK, Ingimarsson J, Knoedler J, Stern K, et al. Over-the-counter alkali agents to raise urine pH and citrate excretion: a prospective crossover study in healthy adults. Urology. 2022; 168: 72–78.
60. Ripa F, Tokas T, Griffin S, Ferretti S, Tur AB, Somani BK. Role of pediatric ureteral access sheath and outcomes related to flexible ureteroscopy and laser stone fragmentation: a systematic review of literature. European Urology Open Science. 2022; 45: 90–98.
61. Chamorro MM, Collado SA, Márquez D. Effectiveness of using Renalof® in the elimination of kidney stones under 10 mm located in the renal-ureteral tract. Open Journal of Nephrology. 2021; 11: 78–92.
62. Saxena A, Sharma RK. Nutritional aspect of nephrolithiasis. Indian Journal of Urology. 2010; 26: 523–530.
63. Dogliotti E, Vezzoli G, Nouvenne A, Meschi T, Terranegra A, Mingione A, et al. Nutrition in calcium nephrolithiasis. Journal of Translational Medicine. 2013; 11: 109.
64. Han H, Segal AM, Seifter JL, Dwyer JT. Nutritional management of kidney stones (nephrolithiasis). Clinical Nutrition Research. 2015; 4: 137–152.
65. de Oliveira LM, Hauschild DB, Leite CD, Baptista DR, Carvalho M. Adequate dietary intake and nutritional status in patients with nephrolithiasis: new targets and objectives. Journal of Renal Nutrition. 2014; 24: 417–422.
66. Grases F, Costa-Bauza A, Prieto RM. Renal lithiasis and nutrition. Nutrition Journal. 2006; 5: 23.
67. Meyers AM, Naicker S. Nephrolithiasis (part 1): epidemiology, causes and pathogenesis of recurrent nephrolithiasis. South African Medical Journal. 2021; 111: 930–933.
68. Wigner P, Grębowski R, Bijak M, Szemraj J, Saluk-Bijak J. The molecular aspect of nephrolithiasis development. Cells. 2021; 10: 1926.
69. Nouvenne A, Meschi T, Guerra A, Allegri F, Prati B, Borghi L. Dietary treatment of nephrolithiasis. Clinical Cases in Mineral and Bone Metabolism. 2008; 5: 135–141.
70. Lightfoot CJ, Wilkinson TJ, Smith AC. Non-pharmacological management of chronic kidney disease. Medicine. 2023; 51: 170–175.
71. Ticinesi A, Nouvenne A, Chiussi G, Castaldo G, Guerra A, Meschi T. Calcium oxalate nephrolithiasis and gut microbiota: not just a gut-kidney axis. A nutritional perspective. Nutrients. 2020; 12: 548.
72. D’Ambrosio V, Ferraro PM, Lombardi G, Friso S, Gambaro G. Unravelling the complex relationship between diet and nephrolithiasis: the role of nutrigenomics and nutrigenetics. Nutrients. 2022; 14: 4961.
73. Worcester EM, Coe FL. Nephrolithiasis. Primary Care: Clinics in Office Practice. 2008; 35: 369–391.
74. Oliveira MC, Goes CR. Mini-review: dietary influency and nutritional treatment in nephrolithiasis. Nutrire. 2022; 47: 14.
75. Soldati L, Bertoli S, Terranegra A, Brasacchio C, Mingione A, Dogliotti E, et al. Relevance of Mediterranean diet and glucose metabolism for nephrolithiasis in obese subjects. Journal of Translational Medicine. 2014; 12: 34.
76. Wasserstein AG. Epidemiology and natural history of nephrolithiasis. Clinical Reviews in Bone and Mineral Metabolism. 2011; 9: 165–180.
77. Cupisti A, D’Alessandro C, Samoni S, Meola M, Egidi MF. Nephrolithiasis and hypertension: possible links and clinical implications. Journal of Nephrology. 2014; 27: 477–482.
78. Meschi T, Nouvenne A, Ticinesi A, Prati B, Guerra A, Allegri F, et al. Dietary habits in women with recurrent idiopathic calcium nephrolithiasis. Journal of Translational Medicine. 2012; 10: 63.
79. Santos FM, Peres AK, Mandotti MR, Peres LA. Metabolic investigation in patients with nephrolithiasis. Einstein. 2017; 15: 452–456.
80. Gambaro G, Reis-Santos JM, Rao N. Nephrolithiasis: why doesn’t our “learning” progress? European Urology. 2004; 45: 547–556.
81. D’Ambrosio V, Moochhala S, Unwin RJ, Ferraro PM. Why is diagnosis, investigation, and improved management of kidney stone disease important? Non-pharmacological and pharmacological treatments for nephrolithiasis. Expert Review of Clinical Pharmacology. 2022; 15: 407–414.
82. Tiselius HG. Medical evaluation of nephrolithiasis. Endocrinology and Metabolism Clinics. 2002; 31: 1031–1050.
83. Zhao A, Dai M, Chen YJ, Chang HE, Liu AP, Wang PY. Risk factors associated with nephrolithiasis: a case-control study in China. Asia Pacific Journal of Public Health. 2015; 27: NP414–NP424.
84. Churchill DN. Urolithiasis-nutritional aspects. Nutrition Research. 1983; 3: 761–771.
85. Hesse A, Siener R. Current aspects of epidemiology and nutrition in urinary stone disease. World Journal of Urology. 1997; 15: 165–171.
86. Remer T, Kalotai N, Amini AM, Lehmann A, Schmidt A, Bischoff-Ferrari HA, et al. Protein intake and risk of urolithiasis and kidney diseases: an umbrella review of systematic reviews for the evidence-based guideline of the German Nutrition Society. European Journal of Nutrition. 2023; 62: 1957–1975.
87. Marra G, Taroni F, Berrettini A, Montanari E, Manzoni G, Montini G. Pediatric nephrolithiasis: a systematic approach from diagnosis to treatment. Journal of Nephrology. 2019; 32: 199–210.
88. Liu YT, Yang PY, Yang YW, Sun HY, Lin IC. The association of nephrolithiasis with metabolic syndrome and its components: a cross-sectional analysis. Therapeutics and Clinical Risk Management. 2017; 13: 41–48.
89. Ciongradi CI, Filip F, Sârbu I, Iliescu Halițchi CO, Munteanu V, Candussi IL. The impact of water and other fluids on pediatric nephrolithiasis. Nutrients. 2022; 14: 4161.
90. Nouvenne A, Ticinesi A, Meschi T. Nephrolithiasis and gastrointestinal tract diseases: can diet intervention help? Practical Gastroenterology. 2013; 116: 27–35.
91. Van den Eynde J, Delpire B, Jacquemyn X, Pardi I, Rotbi H, Gewillig M, et al. Risk factors for acute kidney injury after pediatric cardiac surgery: a meta-analysis. Pediatr Nephrol. 2022; 37: 509–519.
92. Attanasio M. The genetic components of idiopathic nephrolithiasis. Pediatric Nephrology. 2011; 26: 337–346.
93. Allam EA. Urolithiasis unveiled: pathophysiology, stone dynamics, types, and inhibitory mechanisms: a review. African Journal of Urology. 2024; 30: 34.
94. Ziemba JB, Matlaga BR. Epidemiology and economics of nephrolithiasis. Investigative and Clinical Urology. 2017; 58: 299–306.
95. Wal P, Kaushal S, Dwivedi J, Patel P, Sachan P, Srivastava P. Multifunctional roles and phytopharmacological potential of ursolic acid: an invaluable natural nutraceutical agent. Russian Journal of Bioorganic Chemistry. 2025; 51: 1–34.
96. Afsar B, Kiremit MC, Sag AA, Tarim K, Acar O, Esen T, et al. The role of sodium intake in nephrolithiasis: epidemiology, pathogenesis, and future directions. European Journal of Internal Medicine. 2016; 35: 16–19.
97. Soroushzadeh SM, Zareiyan A, Rezaeizadeh H, Karimi M, Arezaei H, Vaghasloo MA. Nutritional viscosity management for renal stones (nephrolithiasis) prevention according to Avicenna’s canon of medicine. Journal of Pharmaceutical Research International. 2019; 31: 1–6.
98. Tamborino F, Cicchetti R, Mascitti M, Litterio G, Orsini A, Ferretti S, et al. Pathophysiology and main molecular mechanisms of urinary stone formation and recurrence. International Journal of Molecular Sciences. 2024; 25: 3075.
99. Meyers AM, Naicker S. Nephrolithiasis (part 2): diagnosis, management and prevention of recurrent nephrolithiasis. South African Medical Journal. 2021; 111: 1042–1045.
100. Hess B, Hasler-Strub U, Ackermann D, Jaeger P. Metabolic evaluation of patients with recurrent idiopathic calcium nephrolithiasis. Nephrology, Dialysis, Transplantation. 1997; 12: 1362–1368.
101. Pedro RN, Aslam AU, Bello JO, Bhatti KH, Philipraj J, Sissoko I, et al. Nutrients, vitamins, probiotics and herbal products: an update of their role in urolithogenesis. Urolithiasis. 2020; 48: 285–301.
102. Abou Chakra M, Dellis AE, Papatsoris AG, Moussa M. Established and recent developments in the pharmacological management of urolithiasis: an overview of the current treatment armamentarium. Expert Opinion on Pharmacotherapy. 2020; 21: 85–96.
103. Hefer M, Huskic IM, Petrovic A, Raguz-Lucic N, Kizivat T, Gjoni D, et al. A mechanistic insight into beneficial effects of polyphenols in the prevention and treatment of nephrolithiasis: evidence from recent in vitro studies. Crystals. 2023; 13: 1070.
104. Nazarian R, Lin N, Thaker S, Yang R, Wong GC, Scotland KB. What causes calcium oxalate kidney stones to form? An update on recent advances. Uro. 2025; 5: 6.
105. Injeyan M, Bidault V, Bacchetta J, Bertholet-Thomas A. Hydration and nephrolithiasis in pediatric populations: specificities and current recommendations. Nutrients. 2023; 15: 728.
106. Roberson D, Sperling C, Shah A, Ziemba J. Economic considerations in the management of nephrolithiasis. Current Urology Reports. 2020; 21: 18.
107. Ticinesi A, Nouvenne A, Borghi L, Meschi T. Water and other fluids in nephrolithiasis: state of the art and future challenges. Critical Reviews in Food Science and Nutrition. 2017; 57: 963–974.
108. Abraham PA, Smith CL. Medical evaluation and management of calcium nephrolithiasis. Medical Clinics of North America. 1984; 68: 281–299.
109. Demoulin N, Aydin S, Gillion V, Morelle J, Jadoul M. Pathophysiology and management of hyperoxaluria and oxalate nephropathy: a review. American Journal of Kidney Diseases. 2022; 79: 717–727.
110. Cameron MA, Pak CY. Approach to the patient with the first episode of nephrolithiasis. Clinical Reviews in Bone and Mineral Metabolism. 2004; 2: 265–278.
111. Rendina D, De Filippo G, Iannuzzo G, Abate V, Strazzullo P, Falchetti A. Idiopathic osteoporosis and nephrolithiasis: two sides of the same coin? International Journal of Molecular Sciences. 2020; 21: 8183.
112. Domrongkitchaiporn S, Sopassathit W, Stitchantrakul W, Prapaipanich S, Ingsathit A, Rajatanavin R. Schedule of taking calcium supplement and the risk of nephrolithiasis. Kidney International. 2004; 65: 1835–1841.
113. Alexander RT, Fuster DG, Dimke H. Mechanisms underlying calcium nephrolithiasis. Annual Review of Physiology. 2022; 84: 559–583.
114. Taylor EN, Curhan GC. Role of nutrition in the formation of calcium-containing kidney stones. Nephron Physiology. 2004; 98: p55–p63.
115. Hess B. Low calcium diet in hypercalciuric calcium nephrolithiasis: first do no harm. Scanning Microscopy. 1996; 10: 547–554; discussion 554–556.
116. Zielinski P, Krupinska J, Wrobel G. The impact of chemical compounds contained in a diet on the development and prevention of urolithiasis. Journal of Elementology. 2021; 26: 163–179.
117. Batanjac J. Nutritional aspects in oxalic urolithiasis. The Scientific Journal Facta Universitatis, Series: Medicine and Biology. 2000; 7: 49–51.
118. Shin S, Srivastava A, Alli NA, Bandyopadhyay BC. Confounding risk factors and preventative measures driving nephrolithiasis global makeup. World Journal of Nephrology. 2018; 7: 129–142.
119. He R, Li P, Lang Y, Zhu B, Yang X, Li J. Associations of obesity, sarcopenia, and sarcopenic obesity with the risk of kidney stones in the US adult: results from NHANES 2011–2018. Urolithiasis. 2025; 53: 111.
120. Rotily M, Léonetti F, Iovanna C, Berthezene P, Dupuy P, Vazi A, et al. Effects of low animal protein or high-fiber diets on urine composition in calcium nephrolithiasis. Kidney International. 2000; 57: 1115–1123.
121. Nouvenne A, Ticinesi A, Allegri F, Guerra A, Guida L, Morelli I, et al. Twenty-five years of idiopathic calcium nephrolithiasis: has anything changed? Clinical Chemistry and Laboratory Medicine. 2014; 52: 337–344.
122. Daudon M, Dessombz A, Frochot V, Letavernier E, Haymann JP, Jungers P, et al. Comprehensive morpho-constitutional analysis of urinary stones improves etiological diagnosis and therapeutic strategy of nephrolithiasis. Comptes Rendus Chimie. 2016; 19: 1470–1491.
123. Rodriguez Cuellar CI, Wang PZ, Freundlich M, Filler G. Educational review: role of the pediatric nephrologists in the work-up and management of kidney stones. Pediatric Nephrology. 2020; 35: 383–397.
124. Dwivedi J, Sachan P, Wal P. A mechanistic approach on structural, analytical and pharmacological potential of Beta-sitosterol: a promising nutraceutical. Current Nutrition & Food Science. 2024; 20: 932–951.
125. Ahmed M, Zareen H, Shaharyar M. Exploring the link between nephrolithiasis and osteoporosis: implications for clinical management and treatment advancements. International Urology and Nephrology. 2025; 57: 2339–2340.
126. Farooq MU, Mustafa SH, Shah MT, Khan MJ, Iftikhar O. Dietary and fluid intake habits in nephrolithiasis patients presented to Ayub Teaching Hospital, Abbottabad. International Journal of Scientific Reports. 2018; 4: 274–277.
127. Dwivedi J, Sachan P, Wal P, Wal A, Rai AK. Current state and future perspective of diabetic wound healing treatment: present evidence from clinical trials. Current Diabetes Reviews. 2024; 20: 45–65.
128. Dwivedi J, Kumar P, Sachan P, Singh C, Saxena B, Wal A, et al. Phyto-pharmacological potential of aegle marmelos (L.) for neurological disorders: progress and prospects. Recent Patents on Food, Nutrition & Agriculture. 2025; 16: 12–30.
129. Madore F, Stampfer MJ, Willett WC, Speizer FE, Curhan GC. Nephrolithiasis and risk of hypertension in women. American Journal of Kidney Diseases. 1998; 32: 802–807.
130. Seitz C, Fajkovic H. Epidemiological gender-specific aspects in urolithiasis. World Journal of Urology. 2013; 31: 1087–1092.
131. Pak CY, Sakhaee K, Crowther C, Brinkley L. Evidence justifying a high fluid intake in treatment of nephrolithiasis. Annals of Internal Medicine. 1980; 93: 36–39.
132. Bargagli M, Ferraro PM, Vittori M, Lombardi G, Gambaro G, Somani B. Calcium and vitamin D supplementation and their association with kidney stone disease: a narrative review. Nutrients. 2021; 13: 4363.
133. Parivar F, Low RK, Stoller ML. The influence of diet on urinary stone disease. The Journal of Urology. 1996; 155: 432–440.
134. Moudi E, Ghaffari R, Moradi A. Pediatric nephrolithiasis: trend, evaluation and management: a systematic review. Journal of Pediatrics Review. 2017; 5: 11–25.
135. Sun K, Zhao N, Shi P, Sun Z, Ye C, Fu L, et al. Early detection and monitoring of nephrolithiasis: the potential of electrochemical sensors. Sensors. 2025; 25: 2547.
136. Ticinesi A, Nouvenne A, Ferraro PM, Folesani G, Lauretani F, Allegri F, et al. Idiopathic calcium nephrolithiasis and hypovitaminosis D: a case-control study. Urology. 2016; 87: 40–45.
137. Mahajan K, Bhagat M, Cherukuri J, Gupta R, Sudershan A, Panjaliya RK. Identification and assessment of non-genetic factors contributing to nephrolithiasis (Kidney Stone) in the Jammu Region. Biosciences Biotechnology Research Asia. 2023; 20: 883–895.
138. Jazayeri SM, Mamaghani ME, Pourmoghaddam A, Azarfar A, Beni MH, Emam SJ. Need for emergent studies on dietary factors among infancy nephrolithiasis. Archives of Italian Urology and Andrology. 2011; 83: 133–135.
139. Dwivedi J, Wal P, Dash B, Ovais M, Sachan P, Verma V. Diabetic pneumopathy—a novel diabetes-associated complication: pathophysiology, the underlying mechanism and combination medication. Endocrine, Metabolic & Immune Disorders-Drug Targets. 2024; 24: 1027–1052.
140. Mennuni G, Serio A, Fontana M, Nocchi S, Costantino C, Tanzi G, et al. Prevention and treatment of nephrolithiasis: a review on the role of spa therapy. Clinical Therapeutics. 2015; 166: 344–356.
141. Mossetti G, Rendina D, De Filippo G, Benvenuto D, Vivona CL, Zampa G, et al. Metabolic syndrome and nephrolithiasis: can we hypotize a common background? Clinical Cases in Mineral and Bone Metabolism. 2008; 5: 114–117.
142. Nackeeran S, Katz J, Ramasamy R, Marcovich R. Association between sex hormones and kidney stones: analysis of the National Health and Nutrition Examination Survey. World Journal of Urology. 2021; 39: 1269–1275.
143. Shabani E, Khorshidi A, Sayehmiri K, Moradi K, Abdolyousefi EN. The effect of nutritional factors on urolithiasis: a case-control study. Journal of Medicine and Life. 2023; 16: 1062–1069.
144. Donsimoni R, Hennequin C, Fellahi S, Troupel S, Le Moel G, Paris M, et al. New aspects of urolithiasis in France. European Urology. 1997; 31: 17–23.
145. Akel M, Cherfan M, Safwan J, Sakr F, Dabbous M, Shamsedeen L, et al. An overview of kidney stone disease in Lebanon. Global Journal of Pharmacology. 2016; 10: 89–97.
146. Jungers P, Joly D, Barbey F, Choukroun G, Daudon M. ESRD caused by nephrolithiasis: prevalence, mechanisms, and prevention. American Journal of Kidney Diseases. 2004; 44: 799–805.
147. Sakhaee K, Adams-Huet B, Moe OW, Pak CY. Pathophysiologic basis for normouricosuric uric acid nephrolithiasis. Kidney International. 2002; 62: 971–979.
148. D’Alessandro C, Ferraro PM, Cianchi C, Barsotti M, Gambaro G, Cupisti A. Which diet for calcium stone patients: a real-world approach to preventive care. Nutrients. 2019; 11: 1182.
149. Lertprapai C, Peerapen P, Thongboonkerd V. Effects of calcium oxalate crystals on neutrophil cellular proteome and functions: implications for nephrolithiasis. Cell Communication and Signaling. 2025; 23: 336.
150. Pahira JJ. Nephrolithiasis: current concepts in medical management. Urologic Radiology. 1984; 6: 74–79.
151. Selvam R, Kalaiselvi P. Oxalate binding proteins in calcium oxalate nephrolithiasis. Urological Research. 2003; 31: 242–256.
152. Ferraro PM, Bargagli M, Trinchieri A, Gambaro G. Risk of kidney stones: influence of dietary factors, dietary patterns, and vegetarian–vegan diets. Nutrients. 2020; 12: 779.
153. Hiatt RA, Ettinger B, Caan B, Quesenberry Jr CP, Duncan D, Citron JT. Randomized controlled trial of a low animal protein, high fiber diet in the prevention of recurrent calcium oxalate kidney stones. American Journal of Epidemiology. 1996; 144: 25–33.
154. Turney BW, Appleby PN, Reynard JM, Noble JG, Key TJ, Allen NE. Diet and risk of kidney stones in the Oxford cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC). European Journal of Epidemiology. 2014; 29: 363–369.
155. Sofia NH, Walter TM, Sanatorium T. Prevalence and risk factors of kidney stone. Global Journal for Research Analysis. 2016; 5: 183–187.
156. Nouvenne A, Ticinesi A, Morelli I, Guida L, Borghi L, Meschi T. Fad diets and their effect on urinary stone formation. Translational Andrology and Urology. 2014; 3: 303–312.
157. Sachan P, Shrivastava P, Goswami M. Revolutionizing the potential of probiotics an evidence-based review. Journal of Ravishankar University. 2024; 37: 60–79.
158. Rodgers AL, Lewandowski S. Effects of 5 different diets on urinary risk factors for calcium oxalate kidney stone formation: evidence of different renal handling mechanisms in different race groups. The Journal of Urology. 2002; 168: 931–936.
159. Robertson WG. Dietary recommendations and treatment of patients with recurrent idiopathic calcium stone disease. Urolithiasis. 2016; 44: 9–26.
160. Barghouthy Y, Corrales M, Somani B. The relationship between modern fad diets and kidney stone disease: a systematic review of literature. Nutrients. 2021; 13: 4270.
161. Boarin M, Villa G, Capuzzi C, Remon D, Abbadessa F, Manara DF. Dietary and lifestyle recommendations for urolithiasis prevention: a systematic literature review. International Journal of Urological Nursing. 2018; 12: 53–70.
162. Kok DJ. The preventive treatment of recurrent stone-formation: how can we improve compliance in the treatment of patients with recurrent stone disease? Urolithiasis. 2016; 44: 83–90.