
Download
REVIEW NEPHROLOGY
The Novel Coronavirus 2019 Epidemic and the Kidneys
Salvadori Maurizio1*, Tsalouchos Aris2
1Careggi University Hospital Florence Italy;
2Department of Medicine; Division of Nephrology and Dialysis Unit, Saints Cosmas and Damian Hospital, Pescia
Abstract
The Severe Acute Respiratory Syndrome Coronavirus 2 is a recent disease that originated in China by the end of 2019. The origins of the disease can be traced to bats, but it has been transmitted to humans, and the inter-human transmission is particularly rampant which has led to a pandemic of unseen proportions. The organ principally involved is the lungs, and severe pneumonia with lack of oxygen leads to fatalities. The aim of this review was to study the involvement of the kidneys with regard to COVID-19 infection and how the disease may affect people on hemodialysis or those who have undergone a kidney transplant. Indeed, the virus, in addition to the lungs, may affect other vascularized organs to a common receptor on lung epithelium and the endothelium of any organ. The kidney, which has a large endothelium surface, is affected, and COVID-19 may lead to acute renal failure. On the other hand, the virus may easily spread among people who are on hemodialysis three times a week. People on hemodialysis may have low immunity, and the virus may have dangerous effects on such people. Finally, renal transplant patients may be easily affected, and the virus may have severe consequences, even death. We will summarize the principal prophylactic measures to be adopted and the therapeutic measures available. Clearly due to the recent occurrence of the pandemic the majority these measures lack a basis in evidence-based medicine and only highlight the efforts to limit COVID-19 induced damage.
Key words: acute kidney injury, coronavirus disease, hemodialysis patients, renal transplant patients, treatment of COVID-19
Received: 22 May 2020; Accepted after Revision: 5 June 2020; Published: 15 June 2020
Author for correspondence: Maurizio Salvadori, Renal Unit, Careggi University Hospital, Viale Pieraccini, Florence, Italy. Email: maurizio.salvadori1@gmail.com
How to cite: Salvadori M and Tsalouchos A. The Novel Coronavirus 2019 Epidemic and the Kidneys. J Ren Hepat Disord. 2020;4(2):11–20.
Copyright: Salvadori M and Tsalouchos A
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0
Introduction
COVID-19 is a disease caused by the new Coronavirus strain, also called Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). The disease was initially identified in the Hubei province of China in late 2019 (1)
There are seven strains of coronavirus that can infect humans. Four of them cause a mild respiratory syndrome in humans and rarely may cause pneumonia, mainly in immunocompromised patients. In the past, two severe epidemics have been caused by two different Coronavirus strains: the Severe Acute Respiratory Syndrome (SARS-CoV) and the Middle East Respiratory Syndrome (MERS-CoV). The mortality rates for these epidemics were 10 and 37%, respectively (2, 3). An in-depth knowledge about these two diseases helped us in understanding some of the characteristics of the SARS-CoV-2. Covid-19 is more contagious than the other Coronavirus strains, has the bat as the source of origin, and its mode of transmission from bat to man has not been completely understood till date. The probability of virus transmission between humans is high and could occur via droplets, feces or direct contact.
The incubation period is between 1 and 10 days. In the vast majority of patients, the disease manifests with a flu-like syndrome, but in several patients the COVID disease has a more severe manifestation, with onset of fever, cough, myalgias, and diarrhea (4). Approximately, 16–20% of patients are affected by a severe syndrome, with bilateral pneumonia and reduced oxygen saturation requiring admission to the intensive care unit (ICU). These patients present with high levels of inflammatory cytokines in the blood as interleukin (IL)-2, IL-6, IL-7, IL-10, and TNFα (5)
COVID 19 and the kidney
The relationship between COVID-19 and the kidney may be divided into three main areas:
-
COVID-19-induced renal disease
-
COVID-19 and dialysis patients
-
COVID-19 and transplant patients
COVID-19-induced renal disease
Although pulmonary infection is the main manifestation in the course of COVID-19, other organs, such as the kidney, may be of interest as well.
Previous studies of SARS and MERS CoV documented the development of acute kidney injury (AKI) in 5–15% of patients with a high mortality rate.
Early reports on COVID-19 documented 3–9% of AKI in patients with COVID infection (6–8). Other data report higher incidence of up to 25% (9).
Two recent reports from New York city noted an incidence of AKI in patients hospitalized with COVID-19 at 31% (10) and of 36.6% (11) respectively.
One study documented that patients on admission affected by leukocyturia, albuminuria, and hematuria, principally when associated with low albumin serum concentration and low antithrombin III concentration, will easily develop AKI (12).
In the renal histopathological analyses of 26 postmortem findings of patients with COVID-19 in China, Su et al. (13) were able to document renal lesions as proximal tubule injury, vacuolar degeneration, and necrosis. By electron microscopy, the same authors were able to find Coronavirus particles in the tubular epithelium and podocytes. In addition, an upregulation of angiotensin converting enzyme 2 (ACE2), the receptor of COVID, was found.
The question remains as to how the COVID-19 virus may enter the renal cells. Another study from Varga et al. (14) has documented that vascular damage in addition to respiratory disease may be observed in the course of COVID-19. Indeed, SARS CoV-2 infects the patient binding to the ACE2 receptor, which is expressed both on the pulmonary epithelium and on the endothelium of several organs, including the kidney. The endothelium involvement may be the way through which the virus enters the cells. Indeed, several studies have documented that during the COVID-19 disease, several organs may be affected in addition to lungs, such as the myocardium and the kidney (15).
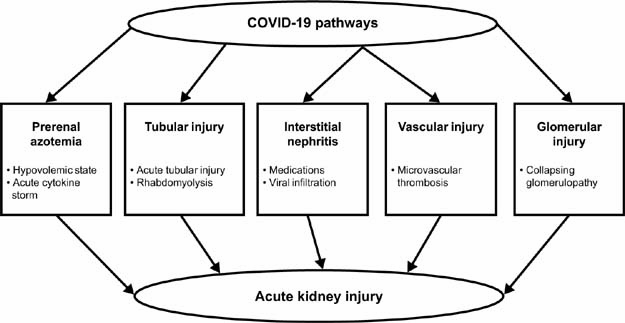
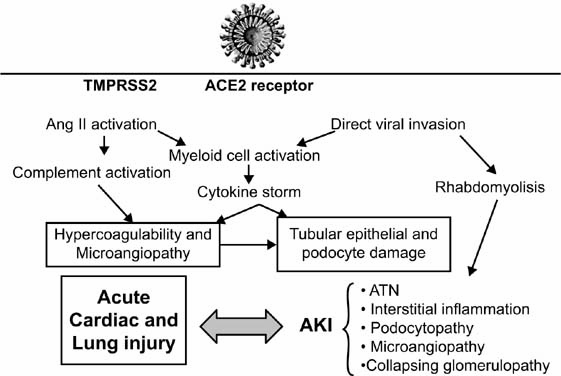
In an observational study, Diao et al. (16) documented that, in a retrospective analysis of 85 patients with COVID-19 infection, confirmed in Wuhan, 23 patients (27.06%) exhibited acute renal failure (ARF), principally related to tubular necrosis, as histologically documented by Su (13). In addition, Diao et al. documented activation of CD68+ macrophages together with complement activation. Further studies have documented that SARS CoV-2 infection, in addition to the release of proinflammatory cytokines, may induce ARF by rhabdomyolysis, hypoxemia, and dehydrated and microvascular thrombosis related to complement activation (17, 18) (Figures 1 and 2). Another cause of ARF in COVID-19 is associated with the collapsing glomerulopathy as documented in two different case reports in which ARF associated with heavy proteinuria affected black patients (19–21). All the patients were black with an APOL1 high-risk genotype.
Figure 1. COVID-19-induced acute kidney injury.
Figure 2. Coronavirus mechanisms of action and damage to the kidney.
TMPRSS2 = transmembrane protease, serine 2; ACE2 = angiotensin-converting enzyme 2; ATN = acute tubular necrosis; AKI = acute kidney injury.
Overall, COVID-19 patients show signs of renal injury including proteinuria (44%), hematuria (26.9%), and increased plasma creatinine (15.5%) (22). The presence of virus particles, both in urine and in renal parenchymal cells, is probably related to the penetration of the virus through the endothelium and the glomerular barrier (23). In another study, Pei et al. (24) documented a renal involvement in 251 out of 333 patients affected by COVID-19. Proteinuria was present in 65.8% of patients and hematuria in 41.7%.
The aforementioned study (11) on COVID-19 patients hospitalized in New York city documented, during univariate and multivariate logistic regression analyses, the risk factors associated with the development of AKI (Table 1).
Table 1. Univariate and multivariate logistic regression analyses of risk factors associated with the development of AKI in COVID-19 patients.
| Variable | Adjusted OR | 95% CI | P |
|---|---|---|---|
| Age (yr) | 1.03 | 1.03–1.04 | <0.001 |
| Male | 1.14 | 0.97–1.33 | 0.10 |
| Diabetes | 1.76 | 1.49–2.07 | <0.001 |
| Hypertension | 1.25 | 1.04–1.50 | 0.02 |
| Cardiovascular disease | 1.48 | 1.22–1.80 | <0.001 |
| Mechanical ventilation | 10.7 | 6.81–16.70 | <0.001 |
| Vasoactive medication | 4.53 | 2.88–7.13 | <0.001 |
To date, the exact mechanism of viral penetration inside the kidney and the subsequent renal damage has not been completely understood. The binding to ACE2 principally in the renal tubules represents the first step (25). The transmembrane protease, serine 2 (TMPRSS2), mediates this first priming step (26, 27). Once inside the kidney, several pathways may be activated as complement activation, cytokine storm, and interstitial inflammation. Viral replication in podocytes could mediate proteinuria (28). Rhabdomyolysis has also been documented in patients with COVID-19 and could contribute to the development of AKI (29).
COVID and dialysis patients
Useful guidelines and suggestions may be obtained from the previous epidemics involving the coronavirus, in particular, the MERS epidemic.
During such epidemics, useful recommendations have been given by the Korean Society of Nephrology (30). According to such recommendations, the following key points should be followed:
-
Patients on hemodialysis with suspected or confirmed MERS-CoV infection should be transferred to a MERS clinic or to a hemodialysis center with facilities, such as isolation rooms.
-
If a patient on hemodialysis is subjected to quarantine due to close contact with a confirmed case, the center should follow the basic principles provided by the prevention authority.
-
Interhospital transfers should be prohibited.
-
All patients and health care workers should follow the standard contact and droplets precautions. A 2-year prospective cohort study (31) documented that a strict patient surveillance and a proper isolation practice prevented secondary transmission of the virus.
To mitigate the risk of COVID-19 in dialysis facilities, the following points have been recently suggested (32):
-
A systemic screening should be adopted for all dialysis patients (symptomatic or not).
-
Patients suspected or confirmed to be affected by COVID-19 should be isolated.
-
Patients should be instructed on the use of face masks. It should be highlighted that controversies on the use and type of masks exist according the different organizations (33–41).
-
Personnel should be provided with protective equipment, including face mask, eye protection, and isolation gowns.
-
Rooms, beds, and dialysis machines should be routinely disinfected.
At the beginning of the COVID-19 spread in Europe, the European Dialysis (EUDIAL) Working Group of the European Renal Association–European Dialysis and Transplant Association (ERA–EDTA) recommended the following measures for the prevention, mitigation, and containment of the emerging SARS-CoV-2 pandemic in hemodialysis centers (42).
Different sets of recommendations are needed for both the healthcare team and the dialysis patients:
-
Recommendations for the health care team:
The health care team should be trained in the use of personal protective equipment.
The health care team should be aware of possible symptoms, so that they can avoid contact with suspected persons.
The health care team should be instructed on the use of protective equipment, such as masks (possible FFP2), goggles, mobcap, and disposable surgical gowns and gloves.
-
Recommendations for dialysis patients:
Patients should be instructed on appropriate hygiene.
Patients should inform the staff on their arrival in case of suspected symptoms.
Patients should be instructed to self-isolate.
Patients’ body temperature should be checked at the start and at the end of the dialysis session.
Symptomatic patients should be dialyzed in an isolated room.
Italy has been deeply affected by the COVID-19 infection, especially Northern Italy.
From an overall population of 643 hemodialysis patients who reported in four dialysis centers in the province of Brescia (Lombardy region), in March 2020, 94 patients (15%) were positive for SARS-CoV-2 RNA.
The data published (43) through univariate analysis and noted as significant causes of death were a history of ischemic heart disease (0.05), fever (0.005), cough (0.01) and shortness of breath at diagnosis (0.001), and elevated C reactive protein (CRP) (0.001). Through multivariate analysis significant factors included fever (0.02), cough (0.05), and CRP at baseline (43).
Patients’ treatment
The drugs used in the treatment of COVID-19 infection to date are:
-
Recombinant soluble ACE2 (44). The rationale behind using hrsACE2 is principally its inhibitory effect on pulmonary infection; however, other organs may also be of affected, especially the capillary walls, the heart, and the kidney.
-
Antiviral treatment. The use of chloroquine and hydroxychloroquine is supported by studies performed in previous SARS infections. Their efficacy in the treatment of COVID-19 infection seems to be relatively poor according to some studies (45, 46). Hydroxychloroquine seems to have an improved immunomodulating effect and a better pharmacological profile. In a small study, hydroxychloroquine, when given in association with antiviral agents, shortens the time to reach the polymerase chain reaction (PCR) negativization (47).
However, the use of both chloroquine and hydroxychloroquine is limited by their myocardial toxicity as recently documented (48). In a recent study (49), both chloroquine and hydroxychloroquine were found to have substantial human toxicity, causing myocardial depression and vasodilatation with impaired myocardial conductivity.
The antiviral therapy uses second-generation antiretroviral drugs in association with lopinavir/ritonavir (50).
Both lopinavir and ritonavir may lead to myocardial toxicity, as they can prolong the QT interval and cause Torsade de Pointes (48). A different antiviral association is the use of darunavir/ritonavir or darunavir/cobicistat with a similar mechanism of action. The antiviral remdesivir is a nucleotide analogue, and its mechanism of action is to incorporate itself in the ribonucleic acid (RNA) chain. Several studies have documented its efficacy (51–53).
Plasma from convalescent patients (54) has been successfully used in the treatment of SARS 1 and MERS. Preliminary data indicate its usefulness in the treatment of SARS-2 as well.
-
Other drugs. One study documented the efficacy of azithromycin when given in association with hydroxychloroquine in reducing the time to achieve PCR negativization (48).
Tocilizumab for its efficacy against IL-6 is an important drug for patients with a severe cytokine storm (55).
Due to the coagulation activity and its involvement in the pathogenesis of the COVID-19-induced lesions, anticoagulant drugs, such as heparin, may play an important role in the treatment of COVID-19 infection (56).
The major limitations in documenting the effective activity of any of the cited drugs is the lack of controlled studies due to the recent occurrence of the disease.
An emerging problem is the possible mutation of the viral genome. In a very recent study on translational medicine (57), the authors have described eight mutations of SARS-CoV-2 in different continents. The virus with mutation in position 14408 was identified in Europe in mid-February. The mutation is RNA dependent and RNA polymerase (RdRp), and the new virus could be resistant to the antiviral agents acting at that level.
From a practical point of view, the Brescia patients on dialysis and with COVID-19 infection have been divided into three groups:
-
Patients on hemodialysis with low symptoms (fever > 27.5, cough without dyspnea and without chest X-ray indications).
If possible treat at home
Antiviral treatment with lopinavir/ritonavir or Darunavir/cobicistat
Hydroxychloroquine for 5 days
Antibiotic protection
No change in dialysis treatment
-
Patients on hemodialysis with severe symptoms (fever > 38°, cough, dyspnea, and/or pneumonia X rays documented).
These patients should be admitted in hospital
Antiviral treatment with lopinavir/ritonavir or Darunavir/ritonavir or Darunavir/cobicistat
Remdesivir should be considered only for patients with a rapid clinical deterioration or severe pneumonia
Hydroxychloroquine
Antibiotic therapy
The dialysis treatment should be made in a quarantine area using dialysis membrane with a high cutoff to remove middle-sized molecules often responsible for the inflammation.
-
Patients hospitalized with clinical deterioration.
Consider deferring patients to ICU
Give dexamethasone at a dose of 20 mg/day
Give Tocilizumab at a dose of 8 mg/Kg of body weight
Consider plasma therapy if available.
COVID-19 and renal transplant patients
There is not much data available on COVID-19 infection in renal transplant patients, and often they are related to case reports (58–60).
Akalin et al. collected data on 36 adult kidney transplant recipients positive for COVID-19 (61) in New York. Patients were treated in different ways according to the severity of their illness. All received reduced immunosuppressive therapy. Overall, there was a high mortality rate (28% at 3 weeks), and all transplanted patients documented a more rapid clinical progression than the general population affected by COVID-19.
In a different study (62), 10 kidney transplant patients tested positive for SARS-CoV-2 by PCR. Among them, three patients died (30%) and five developed acute kidney injury (AKI) (50%).
Better outcomes were observed at Columbia University Hospital, where 15 kidney transplant patients required hospitalization for confirmed COVID-19 (63). Six patients (40%) had AKI and four patients required intubation or mechanical ventilation. Two patients died. The authors themselves do not understand the reason for this lower mortality rate with respect to similar patients in the same area (61). The small patient number does not allow a statistical comparison.
A study from Iran (64) described 12 renal transplant patients with COVID-19 infection. In this group, eight patients died and four were discharged.
Twenty kidney transplant patients were admitted for SARS-CoV-2 pneumonia in the Brescia hospital (65): six patients developed AKI and five patients (25%) died. The study confirms a rapid clinical deterioration in renal transplant patients. Transplant patients are at a higher risk of developing a severe COVID-19 infection. To reduce this risk, several prophylactic and therapeutic measures should be adopted:
-
Prophylaxis. As aforementioned, a careful and repeated washing of hands with soap and alcohol is recommended, both for patients and the health care team.
Vaccinations as antipneumococcal are similarly recommended to avoid preventable infections.
Transplant patients should not travel, and the same holds good for their partners and family. Lockdown at home is recommended in areas with a high rate of COVID-19 spread.
Patients should wear a mask covering their mouth and nose when venturing out of home, and are recommended to stay at a distance from other people. As previously mentioned, the frequency of which mask should be used is open to wide discussion.
Prophylactic measures should be particularly adopted for patients with mild fever or cough and for those who had been in close contact with people suspected to have had Covid-19 in the last 14 days (66). In the case of patients with symptoms, they should stay in a protected site and should follow the guidelines that are continuously updated by the Center for Disease Control and Prevention (CDC) (67).
-
Modification of immunosuppressant drugs. Different approaches to this very important issue do exist. No all are concordant.
The Descartes Group of the ERA–EDTA (68) suggests the following guidelines:
-
In the case of asymptomatic patients without COVID-19 infection, there is no need to modify immunosuppressive treatment.
-
In the case of patients with mild disease:
-
If patients are on triple therapy, they should stop mycophenolic acid/ azathioprine or mammalian target of rapamycin inhibitors (mTORIs). Patients should remain on calcineurin inhibitor (CNI) and steroids.
-
If patients are on dual therapy, generally there is no need to change, but if dual therapy is CNI + MPA/mTORIs, the latter can be substituted with steroids. Reduce calcineurin inhibitors (CNIs) to the lowest possible levels considering the immunological risk
-
-
In the case of patients with COVID-19 pneumonia and oxygen saturation over 94–95%:
-
Patients at high risk for age or for co-morbidities, such as diabetes, cardiac disease, history of smoking, BMI > 30 kg/m2 , estimated glomerular filtration rate (eGFR) < 30 mL/min, should stop MPA/AZA/mTORIs, should stop CNIs and increase or start steroids at 15–25 mg/day.
-
High-risk patients should not stop MPA/AZA/mTORIs, and they should be maintained on dual therapy with CNIs and steroids, reducing the CNI dosing.
-
In patients on antiviral treatment, CNI should be stopped.
-
-
In the case of patients with severe COVID-19 pneumonia, with oxygen saturation under 94% or needing mechanical ventilation:
-
All immunosuppressants must be stopped. Steroids should be started or continued at 15–25 mg/day. CNI might be continued at very low dosing in patients at high risk for rejection
-
-
-
Treatment of transplant patients with COVID-19. We have already mentioned the drugs used for COVID-19 infection. The same drugs are used for kidney transplant patients with the following considerations (69):
-
Asymptomatic/paucisymptomatic transplant patients without dyspnea and with negative chest X rays.
In addition to the modifications to the immunosuppressive treatment, these patients should receive:
Lopinavir/ritonavir or
Darunavir/ritonavir or
Darunavir/cobicistat
In addition to the antiviral treatment, they should receive:
Hydroxychloroquine for 5 days at a dose in accordance with the eGFR
Azithromycin 500 mg/day
-
Patients with severe symptoms with dyspnea and/or positive chest X rays.
These patients should receive the same antiviral treatment.
Remdesivir should be considered as a first-line treatment in patients with rapid deterioration, severe pneumonia, and needing mechanical ventilation.
In the case of rapid deterioration, treatment with tocilizumab should also be considered. Tocilizumab dose should be decided according to body weight (55).
-
Due to the interaction between hydroxychloroquine, ritonavir, cobicistat, and the immunosuppressants, patients receiving such antiviral drugs must stop mTORIs and CNIs. As hydroxychloroquine is given for only 5 days, it is only necessary to check for the through levels of CNIs.
-
-
Renal transplantation from a cadaver or living donor during the COVID-19 pandemic. Due to the scarcity of data, it is not to date clear as to whether patients on waiting list and recent COVID-19 infection may be safely transplanted. The general recommendation is that before reentering the waiting list, the patient should have two PCR negative tests.
The same recommendation should be made both for living and cadaveric donors.
Even if the risk has not been verified, RNA viral transmission has been documented in 15% of transplants in a study (69).
The American Society of Transplantation developed the following tables (Tables 2 and 3) for a better understanding about new transplantations.
As a consequence, they should be recommended as follows:
-
Living donors who have recently travelled to areas with high virus spread or who have contacted people afflicted with COVID-19 should postpone the donation by at least 3 weeks and should have a negative PCR.
-
Cadaveric donors affected with COVID-19 must be discharged.
-
Cadaveric donors at epidemiological risk for COVID-19 should be ruled out for donations that are not considered life saving.
-
Living and cadaveric donors with a past history of COVID-19 should have been cured at least 1 month prior to transplantation, and the use of their organs should be discussed before transplantation.
-
The adoption of such measures has reduced the transplantation activity. Preliminary Italian data show a reduction of procured organs by about 25% in the first 4 weeks of the COVID-19 outbreak (70).
Table 2. Exposure and clinical screening of potential donors with COVID-19.
Epidemiological screening
|
Clinical screening
|
Table 3. Donor classification for donor-derived COVID-19 based on clinical symptoms and epidemiological screening of Table 1.
High risk
|
Intermediate risk
|
Intermediate risk
|
Low risk
|
Conclusions
The interrelationship between COVID-19 and the kidneys is probably more complex than previously suspected. The localization of angiotensin-converting enzyme (ACE)2 receptor, which is the binding site of the virus on the epithelial surface, exposes many organs as possible targets of COVID-19.
In the case of kidney, several pathways have been identified, which can lead to acute renal injury. The presence of AKI in a patient with severe pulmonary distress may represent a clear cause leading to death.
A particular condition is represented by the hemodialysis patients who may easily be affected by COVID-19 infection, either because the virus may easily infect them or because they are generally older with reduced immune response.
Renal transplant patients represent a high-risk population because they are immunosuppressed.
To date, we do not have enough epidemiological data concerning transplant patients, but from the data we have, a high predisposition towards AKI or death seems to be documented.
Treatment still represents a crucial problem. The lack of evidence-based treatments and of randomized controlled trials makes any possible treatment the object of controversies.
To date, oxygen, lockdown, and protective measures seem to be the only safe methods. While waiting for a vaccine or the results of controlled trials, we have to carefully monitor our patients, and treat them with the available drugs with extreme caution.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
REFERENCES
1. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020 Feb 7;323(11):1061–9. 10.1001/jama.2020.1585
2. World Health Organization. Summary of probable SARS cases with onset of illness from 1 November 2002 to 31 July 2003 [Internet]. [cited
3. World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV). November 2019 [Internet]. [cited
4. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506. 10.1016/S0140-6736(20)30183-5
5. Center for Disease Control and Prevention. Frequently asked questions and answers: Coronavirus Disease-2019 (COVID 19) and children [Internet]. [cited
6. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study Lancet. 2020 Feb 15;395(10223):507–13. 10.1016/S0140-6736(20)30211-7
7. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382:1708–20. 10.1056/NEJMoa2002032
8. Cheng Y, Luo R, Wang K, Zhang M, Wang Z, Dong L, et al. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020 May;97(5):829–38. 10.1016/j.kint.2020.03.005
9. Naicker S, Yang CW, Hwang SJ, Liu BC, Chen JH, Jha V. The novel coronavirus 2019 epidemic and kidneys. Kidney Int. 2020 May;97(5):824–8. 10.1016/j.kint.2020.03.001
10. Cummings MJ, Baldwin MR, Abrams D, Jacobson SD, Meyer BJ, Balough EM, et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet. 2020 May 19. 10.1016/S0140-6736(20)31189-2. Online ahead of print.
11. Hirsch JS, Ng JH, Ross DW, Sharma P, Shah HH, Barnett RL, et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020 May 13;S0085-2538(20)30532-9. 10.1016/j.kint.2020.05.006. Online ahead of print.
12. Gross O, Moerer O, Weber M, Huber TB, Scheithauer S. COVID-19-associated nephritis: Early warning for disease severity and complications? Lancet. 2020 May 16;395(10236):e87–e88. 10.1016/S0140-6736(20)31041-2
13. Su H, Yang M, Wan C, Yi LX, Tang F, Zhu HY, et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020 Apr 9;S0085-2538(20)30369-0. 10.1016/j.kint.2020.04.003
14. Varga Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, Zinkernagel AS. Endothelial cell infection and endotheliitis in COVID-19. Lancet. 2020;395:1417–18. 10.1016/S0140-6736(20)30937-5
15. Dong N, Cai J, Zhou Y, Liu J, Li F. End-stage heart failure with COVID-19: Strong evidence of myocardial injury by 2019-nCoV. JACC Heart Fail. 2020 Apr 7;S2213-1779(20)30200-6.
16. Diao B, Wang C, Wang R, Feng Z, Tan Y, Wang H, et al. Human kidney is a target for novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Infection. medRxiv. 10.1101/2020.03.04.20031120. e-published ahead of print
17. Yalameha B, Roshan B, Bhaskar L, Mohmoodnia L. Perspectives on the relationship of renal disease and coronavirus disease 2019. J Nephropharmacol. 2020;9(2):e22.
18. Batlle D, Soler MJ, Sparks MA, Hiremath S, South AM, Welling PA. Acute kidney injury in COVID-19: Emerging evidence of a distinct pathophysiology. JASN. May 2020;ASN.2020040419. 10.1681/ASN.2020040419. published online ahead of print
19. Larsen CP, Bourne TD, Wilson JD, Saqqa O, Sharshir MA. Collapsing glomerulopathy in a patient with coronavirus disease 2019 (COVID-19). Kidney Int Rep. 2020 Apr 9. 10.1016/j.ekir.2020.04.002. Online ahead of print.
20. Peleg Y, Kudose S, D’Agati V, Siddall E, Ahmad S, Kisselev S, et al. Acute kidney injury due to collapsing glomerulopathy following COVID-19 Infection. Kidney Int Rep. 2020 Apr 28. 10.1016/j.ekir.2020.04.017. Online ahead of print.
21. Genovese G, Friedman DJ, Ross MD, Lecordier L, Uzureau P, Freedman BI, et al. Association of trypanolytic ApoL1 variants with kidney disease in African Americans. Science. 2010 Aug 13;329(5993):841–5.
22. Hong XW, Chi ZP, Liu GY, Huang H, Guo SQ, Fan Jr, et al. Analysis of early renal injury in COVID-19 and diagnostic value of multi-index combined detection. MedRxiv. 2020. 10.1101/2020.03.07.20032599
23. Xie Z, Bao J, Cai Z, Liu S, Chen H, Qi J, et al. Clinical characteristics of 60 COVID-19-infected patients with or 2 without renal injury in Hangzhou, China [Internet]. Available from: SSRN: https://ssrn.com/abstracr=3541126
24. Pei G, Zhang Z, Peng J, Liu L, Zhang C, Yu C, et al. Renal involvement and early prognosis in patients with COVID-19 pneumonia. JASN. 2020;31(6):1157–65. 10.1681/ASN.2020030276
25. Jia HP, Look DC, Shi L, Hickey M, Pewe L, Netland J, et al. ACE2 receptor expression and severe acute respiratory syndrome coronavirus infection depend on differentiation of human airway epithelia. J Virol. 2005;79:14614–21. 10.1128/JVI.79.23.14614-14621.2005
26. Wilson PC, Wu H, Kirita Y, Uchimura K, Ledru N, Rennke HG, et al. The single-cell transcriptomic landscape of early human diabetic nephropathy. Proc Natl Acad Sci U S A. 2019;116:19619–25. 10.1073/pnas.1908706116
27. Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, function, and antigenicity of the SARS-CoV-2 Spike glycoprotein. Cell. 2020;181:281–292.e6. 10.1016/j.cell.2020.02.058
28. Ye M , Wysocki J, William J, Soler MJ, Cokic I, Batlle D. Glomerular localization and expression of angiotensin-converting enzyme 2 and angiotensin-converting enzyme: Implications for albuminuria in diabetes. J Am Soc Nephrol. 2006 Nov;17(11):3067–75. 10.1681/ASN.2006050423
29. Suwanwongse K, Shabarek N. Rhabdomyolysis as a presentation of 2019 novel coronavirus disease. Cureus. 2020 Apr 6;12(4):e7561. 10.7759/cureus.7561
30. Park HC, Lee YK, Lee SH, Yoo KD, Jeon HJ, Ryu DR, et al. Middle east respiratory syndrome clinical practice guideline for hemodialysis facilities. Kidney Res Clin Pract. 2017 Jun;36(2):111–16. 10.23876/j.krcp.2017.36.2.111
31. Park HC, Lee SH, Kim J, Kim DH, Cho AJ, Jeon HJ, et al. Effect of isolation practice on the transmission of middle east respiratory syndrome coronavirus among hemodialysis patients: A 2-year prospective cohort study. Medicine (Baltimore). 2020 Jan;99(3):e18782. 10.1097/MD.0000000000018782
32. Alan S, Kliger AS, Silberzweig J. Mitigating risk of COVID-19 in dialysis facilities. CJASN. 2020;15:707–9. 10.2215/CJN.03340320
33. Feng S, Shen C, Xia N, Song W, Fan M, Cowling BJ. Rational use of face masks in the COVID-19 pandemic [Internet]. Available from: www.thelancet.com/resiratory Published Online
34. WHO. Coronavirus disease (COVID-19) advice for the public: When and how to use masks. 2020 [Internet]. [cited
35. State Council, China. Guidelines for the selection and use of different types of masks for preventing new coronavirus infection in different populations 2020 (in Chinese) [Internet]. Feb 5, 2020. [cited
36. The Department of Health, Hong Kong. Guidelines on prevention of coronavirus disease 2019 (COVID-19) for the general public. March 13, 2020 [Internet]. [cited
37. Ministry of Health, Singapore. Updates on COVID-19 (coronavirus disease2019) local situation [Internet]. [cited
38. Ministry of Health, Labour and Welfare, Japan. Q & A on coronavirus 2019(COVID-19): When should I wear a facemask? [Internet]. 2020 [cited
39. CDC. Coronavirus Disease 2019 (COVID-19): Steps to prevent illness [Internet]. [cited
40. National Health Service. Are face masks useful for preventing coronavirus? [Internet]. 2020 [cited
41. Federal Ministry of Health, Germany. Daily updates on the coronavirus: Is wearing a surgical mask, as protection against acute respiratory infections, useful for members of the general public? [Internet]. 2020 [cited
42. Basile C, Combe C, Pizzarelli F, Covic A, Davenport A, Kanbay M, et al. Recommendations for the prevention, mitigation and containment of the emerging SARS-CoV-2 (COVID-19) pandemic in haemodialysis centres. Nephrol Dial Transplant. 2020;35:737–41. 10.1093/ndt/gfaa069
43. Alberici F, Delbarba E, Manenti C, Econimo L, Valerio F, Pola A, et al. A report from the Brescia Renal COVID Task Force on the clinical characteristics and short-term outcome of hemodialysis patients with SARS-CoV-2 infection. Kidney Int. 2020. epub ahead of print 10.1016/j.kint.2020.04.030
44. Alhenc-Gelas F, Drueke TB. Blockade of SARS-CoV-2 infection by recombinant soluble ACE2. Kidney Int. 2020;97:1091–3. 10.1016/j.kint.2020.04.009
45. Multicenter Collaboration Group of Department of Science and Technology of Guangdong Province and Health Commission of Guangdong Province for chloroquine in the treatment of novel coronavirus pneumonia. [Expert consensus on chloroquine phosphate for the treatment of novel coronavirus pneumonia]. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43:185–8.
46. Cortegiani A, Ingoglia G, Ippolito M, Einav S. Chloroquine for COVID-19: Rationale, facts. Hopes Crit Care. 2020 May 8;24(1):210–13. 10.1186/s13054-020-02932-4
47. Gautret P, Lagier JC, Parola P, Hoang VT, Meddeb L, Mailhe M, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open label non-randomized clinical trial [e-pub ahead of print]. Int J Antimicrob Agents. 2020 Mar 20:105949. 10.1016/j.ijantimicag.2020.105949. Epub ahead of print
48. Naksuk N, Lazar S, Peeraphatdit TB. Cardiac safety of off-label COVID-19 drug therapy: A review and proposed monitoring protocol. Eur Heart J Acute Cardiovasc Care. 2020 May 6;2048872620922784. 10.1177/2048872620922784. Online ahead of print.
49. Erickson TB, Chai PR, Boyer EW. Chloroquine, hydroxychloroquine and COVID-19. Toxicol Commun. 2020;4(1):40–2. 10.1080/24734306.2020.1757967. Epub 2020 Apr 30
50. Cao B, Wang Y, Wen D, Liu W, Wang J, Fan G, et al. A trial of lopinavir-ritonavir in adults hospitalized with severe Covid-19 [e-pub ahead of print]. N Engl J Med. 2020 May 7;382(19):1787–99.
51. Sheahan TP, Sims AC, Leist SR, Schäfer A, Won J, Brown AJ, et al. Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV. Nat Commun. 2020 Jan 10;11(1):222–36. 10.1038/s41467-019-13940-6
52. de Wit E, Feldmann F, Cronin J, Jordan R, Okumura A, Thomas T, et al. Prophylactic and therapeutic remdesivir (GS-5734) treatment in the rhesus macaque model of MERS-CoV infection. Proc Natl Acad Sci U S A. 2020;117(12):6771–6. 10.1073/pnas.1922083117
53. Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020;30(3):269–71. 10.1038/s41422-020-0282-0
54. Bloch EM, Shoham S, Casadevall A, Sachais BS, Shaz B, Winters JL, et al. Deployment of convalescent plasma for the prevention and treatment of COVID-19. J Clin Invest. 2020 Apr 7;138745. 10.1172/JCI138745. Online ahead of print.
55. Frey N, Porter D. Cytokine release syndrome with chimeric antigen receptor T cell therapy. Biol Blood Marrow Transplant. 2019;25(4):e123–7. 10.1016/j.bbmt.2018.12.756
56. Porfidia A, Pola R. Venous thromboembolism and heparin use in COVID-19 patients: Juggling between pragmatic choices, suggestions of medical societies and the lack of guidelines. J Thromb Thrombolysis. 2020 May 16;1. 10.1007/s11239-020-02139-y. Online ahead of print.
57. Pachetti M, Marini B, Benedetti F, Fabiola Giudici F , Elisabetta Mauro E , Paola Storici P, et al. Emerging SARS-CoV-2 mutation hot spots include a novel RNA-dependent-RNA polymerase variant. Transl Med. 2020 Apr 22;18(1):179. 10.1186/s12967-020-02344-6
58. Zhu L, Xu X, Ma K, Yang J, Guan H, Chen S, et al. Successful recovery of COVID-19 pneumonia in a renal transplant recipient with long-term immunosuppression. Am J Transplant. 2020 Mar 17;10:1–5. 10.1111/ajt.15869
59. Guillen E, Pineiro GJ, Revuelta I, Rodriguez D, Bodro M, Moreno A, et al. Case report of COVID-19 in a kidney transplant recipient: Does immunosuppression alter the clinical presentation? Am J Transplant. 2020 Mar 20. 10.1111/ajt.15874. Online ahead of print.
60. Gandolfini I, Delsante M, Fiaccadori E, Zaza G, Manenti L, Degli Antoni A, et al. COVID-19 in kidney transplant recipients. Am J Transplant. 2020 Mar 31. 10.1111/ajt.15891. Online ahead of print.
61. Akalin E, Azzi Y, Bartash R, Seethamraju H, Parides M, Hemmige V, et al. Covid-19 and kidney transplantation. N Engl J Med. 2020 Apr 24;NEJMc2011117. 10.1056/NEJMc2011117. Online ahead of print.
62. Nair V, Jandovitz N, Hirsch JS, Nair G, Abate M, Bhaskaran M, et al. COVID-19 in kidney transplant recipients. Am J Transplant. 2020 Apr 29. 10.1111/ajt.15967. Online ahead of print.
63. Columbia University. Kidney transplant program early description of coronavirus 2019 disease in kidney transplant recipients in New York. J Am Soc Nephrol. 2020 Apr 21;ASN.2020030375. 10.1681/ASN.2020030375. Online ahead of print.
64. Abrishami A, Samavat S, Behnam B, Arab-Ahmadi M, Nafar M, Taheri MS, et al. Clinical course, imaging features, and outcomes of COVID-19 in kidney transplant recipients. Eur Urol. 2020 May 6;S0302-2838(20)30332-8. 10.1016/j.eururo.2020.04.064. Online ahead of print.
65. Alberici F, Delbarba E, Manenti C, Econimo L, Valerio F, Pola A. Management of patients on dialysis and with kidney transplant during SARS-COV-2 (COVID-19) pandemic in Brescia, Italy. Kidney Int Rep. 2020 Apr 4;5(5):580–5. 10.1016/j.ekir.2020.04.001
66. Michaels MG, La Hoz RM, Danziger-Isakov L, Blumberg EA, Kumar D, Green M, et al. Coronavirus disease 2019: Implications of emerging infections for transplantation. Am J Transplant. 2020 Feb 24. 10.1111/ajt.15832. Online ahead of print.
67. Centre for Disease Control. Follow updated guidelines [Internet]. [cited
68. ERA-EDTA. WG Descartes expert opinion regarding the management of immunosuppressive medication for kidney transplant patients during the COVID-19 pandemic [Internet]. [cited
69. American Society of Transplantation. 2019-nCoV (Coronavirus): FAQs for organ donation and transplantation [Internet]. Updated March 30, 2020 [cited
70. Angelico R, Trapani S, Manzia TM, Lombardini L, Tisone G, Cardillo M. The COVID-19 outbreak in Italy: Initial implications for organ transplantation programs. Am J Transplant. 2020 Apr 3. 10.1111/ajt.15904. Online ahead of print.