
Download
ORIGINAL ARTICLE
Paradigm Shift in Etiology of Upper Gastrointestinal Bleed in Emergency Department
Tarana Gupta*, Sandeep Goyal
Department of Medicine, Pt B D Sharma University of Health Sciences, Rohtak, India
Abstract
Acute upper gastrointestinal (UGI) bleed is an emergency requiring immediate intervention. Recent data have shown peptic ulcer disease (PUD) to be the commonest cause of UGI bleed. We aimed to evaluate all patients with UGI bleed reporting in the emergency department. A cross-sectional, observational study from a tertiary care center; evaluated all patients with UGI bleed presenting to the outpatient and emergency departments between December 2017 and December 2018. A total of 356 patients with UGI bleed were enlisted for diagnostic and therapeutic endoscopy. Variceal bleed was present in 231 (65%) [cirrhosis 217 (61%) vs noncirrhotic 14 (4%)] patients, nonvariceal bleed was present in 93 (26%) [cirrhosis 22(6%) vs noncirrhotic 71(20%)] patients, and no cause was determined in 32 (9%) patients. Among cirrhotic patients, alcoholic liver disease (n = 172) was the most common, followed by cryptogenic cirrhosis (n = 32), and cirrhosis related to Hepatitis B (n =7) and hepatitis C virus (n =22), and AIH (n = 6). Among variceal noncirrhotic causes, noncirrhotic portal hypertension was present in 14 patients. In the noncirrhotic, nonvariceal group, causes of UGI bleed included esophagitis (n = 26), erosive gastritis (n = 9), and Mallory Weiss Tear (n = 7), followed by PUD (n = 23), carcinoma stomach (n = 3), carcinoma esophagus (n = 2), and duodenal polyp (n = 1). Nonvariceal cirrhotic patients had portal hypertensive gastropathy (n = 8), PUD (n = 5), duodenal erosions (n = 1), esophagitis (n = 7), and antral varix (n = 1). Interestingly, even in the nonvariceal group, alcohol was the underlying cause of UGI bleed in majority of the patients with esophagitis and erosive gastritis. Alcohol was the commonest cause of UGI bleed in majority of the cases with or without chronic liver disease, followed by PUD in small numbers in the emergency department.
Key words: alcoholic liver disease, peptic ulcer disease, upper gastrointestinal bleed
Received: 8 December 2020; Accepted after Revision: 14 January 2021; Published: 16 March 2021.
Author for correspondence: Tarana Gupta, MD, DM Hepatology, Professor, Department of Medicine, Post Graduate Institute of Medical Sciences (PGIMS), Rohtak, India. Tel.: 9914048899. Email: taranagupta@gmail.com
How to cite: Gupta T and Goyal S. Paradigm Shift in Etiology of Upper Gastrointestinal Bleed in Emergency Department. J Ren Hepat Disord. 2021;5(1): 14–18.
Doi: https://dx.doi.org/10.15586/jrenhep.v5i1.93
Copyright: Gupta T, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Upper gastrointestinal (UGI) bleed is an important cause of emergency medical admission and mortality. It requires immediate resuscitation and interventions for improved outcomes. The epidemiological data help us in assessing the burden, etiology, and severity of the disease. Peptic ulcer disease (PUD) had been one of the commonest causes in almost 60–75% and variceal bleed in 6–14% of upper Gastrointestinal bleed in Western studies (1, 2). Indian data have also shown PUD in 20–55% and variceal bleed in 12–55% of emergency UGI bleed cases (3–6). The increasing prevalence of chronic liver disease due to viral hepatitis, alcohol, and nonalcoholic fatty liver disease has resulted in complications of portal hypertension. Gastrointestinal endoscopy remains the diagnostic and therapeutic procedure of choice for upper gastrointestinal bleed (UGI Bleed). The present study was aimed to assess the etiology of UGI bleed in patients reporting in the emergency department in a tertiary care hospital.
Methods
This observational, cross-sectional study included all patients presenting with UGI bleed in the emergency department in the Post Graduate Institute of Medial Sciences, Rohtak, Haryana, from December 2017 to December 2018. All patients aged >12 years, presenting with either hematemesis or melena in the emergency department were included in the study. Clinical data and endoscopic findings were collected for all the patients. Written informed consent was collected from all the patients.
Statistical analysis
Quantitative variables were presented as mean with standard deviation/range and qualitative variables as proportions with percentages. Categorical variables were analyzed using the Chi square test. Quantitative variables were expressed as mean (range) and compared using the Student t-test. P value <0.05 was considered significant. Data were analyzed using SPSS v21.0 (IBM, USA).
Results
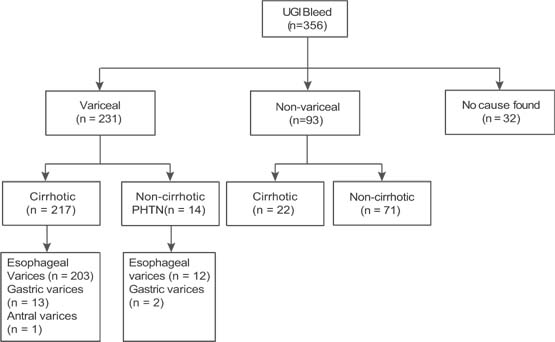
A total of 356 patients underwent upper GI endoscopy for UGI bleed referred from the outpatient department or the emergency department. Of these 356 patients (Figure 1), variceal bleed was present in 231 (65%) patients, which included 217 (61%) patients with cirrhosis of liver and 14 (4%) patients with noncirrhotic portal hypertension (NCPH). Among 217 patients of cirrhosis, alcohol was the most common cause of chronic liver disease in 172 patients, followed by cryptogenic cirrhosis in 32, chronic hepatitis-C-related cirrhosis in 22, chronic hepatitis-B-related cirrhosis in seven, and autoimmune- related cirrhosis in six patients. Of the 217 cirrhotic variceal bleed patients, 203 (94%) patients had bleed due to esophageal varices, 13 (6%) had fundal varices, and one had antral varices. Among 14 patients of NCPH, UGI bleed was due to esophageal varices in 12 (86%) patients and gastric varices in two (14%) patients.
Figure 1: Distribution of variceal and nonvariceal causes of upper GI bleed.
Among 93 patients with nonvariceal causes of UGI bleed, the majority were noncirrhosis (n = 71) and only 22 had cirrhosis of liver (Figure 1). Among the noncirrhotic, nonvariceal group (n = 71), alcoholism was present in 26 patients. Overall, the causative lesion was esophagitis in 26, erosive gastritis in nine, Mallory Weiss Tear in seven, followed by PUD in 23, carcinoma stomach in three, carcinoma esophagus in two, and duodenal polyp in one patient (Table 1). Nonvariceal cirrhotic patients (n = 22) had portal hypertensive gastropathy in eight, PUD in five, duodenal erosions in one, esophagitis in seven, and antral varix in one patient (Table 1). Alcoholic liver disease was present in 10 patients in the nonvariceal cirrhosis group.
Table 1: Spectrum of upper GI bleed presenting in emergency department in the nonvariceal group (n = 93).
| Nonvariceal causes of UGI bleed | n = 93 |
|---|---|
| Cirrhosis (n = 22) | |
| PHG | 8 |
| Esophagitis | 7 |
| Duodenal ulcer | 5 |
| Duodenal erosions | 1 |
| Antral varix | 1 |
| Noncirrhotics (n = 71) | |
| Peptic ulcer | 23 |
| Esophagitis | 26 |
| Erosive gastritis | 9 |
| MW Tear | 7 |
| Carcinoma stomach | 3 |
| Carcinoma esophagus | 2 |
| Duodenal polyp | 1 |
PHG, Portal hypertensive gastropathy; MW tear, Mallory–Weiss tear.
No cause of UGI bleed could be determined in 32 (9%) patients.
The mean age of patients was 40 years in the cirrhosis group and 35 years in the noncirrhotic group. The cirrhosis group had more males as compared to the noncirrhotic group (81% vs 70%, P = 0.07) (Table 2). Alcohol was the most common etiology of the cirrhosis group as compared to the noncirrhotic group (72% vs 30%, P = 0.03). Number of bleeding episodes were less in the cirrhosis group as compared to the noncirrhotic group (6.3 vs 9, P = 0.83) although volume of bleed per episode was significantly more in the cirrhosis group as compared to the noncirrhosis group (300 vs 100, P = 0.04). The mean bilirubin values were significantly higher in cirrhosis than in noncirrhosis patients.
Table 2: Baseline characteristics among cirrhosis and noncirrhosis patients.
| Variables | Cirrhosis (n = 239) | Noncirrhosis (n = 85) | P value |
|---|---|---|---|
| Age (years) | 40 (17–70) | 35 (10–80) | 0.07 |
| Male, n (%) | 195 (81%) | 60 (70%) | 0.06 |
| Alcohol, n (%) | 172 (72%) | 26 (30%) | 0.03 |
| Hb (gm/dL) | 6.3 (3.5–10.5) | 9.0 (5.4–13.2) | 0.05 |
| Bleeding episodes (average per patient) | 1.6 (1–3) | 2 (1–4) | 0.83 |
| Volume of bleed per episode (mL) | 300 (100–500) | 100 (50–250) | 0.04 |
| Mean Bilirubin (mg/dL) | 7.2 (1.3–37) | 2.5 (1.1–10.1) | 0.03 |
Hb, hemoglobin; data were expressed as mean (range) otherwise expressed.
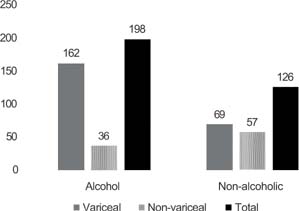
Of a total of 324 patients in which a cause of upper GI bleed could be ascertained, majority of them were alcoholic (n = 198, 61%) with 162 (82%) having variceal bleed and 36 (18%) having nonvariceal causes of UGI bleed (Figure 2). Of the remaining 126 patients, 69 had variceal bleed and 57 had nonvariceal causes of bleed.
Figure 2: Spectrum of upper GI bleed in alcoholics (n = 198) and nonalcoholics (n = 126).
Discussion
Upper GI bleed is traditionally defined as bleeding from the gastrointestinal tract that is proximal to the ligament of Treitz. It presents as hematemesis, melaena, or less predictively as melaenemesis (coffee ground vomiting), and has had a stable mortality of 10% worldwide, in spite of several novel approaches to its treatment including the use of endo-clot powder spray, tranexamic acid, and interventional endoscopic procedures, among others. Of the major causes such as esophagitis, varices, PUD, and erosive gastritis, variceal bleeding is known to carry a higher fatality in the absence of timely intervention.
Our study showed portal hypertension to be the most common cause of UGI bleed presenting as variceal bleed.
Moreover, cirrhosis supersedes NCPH in portal hypertensive bleeds. Furthermore, among nonvariceal causes of UGI bleed, esophagitis and erosive gastritis outnumbered the bleeds due to PUD. Collectively, alcohol emerged as the most common cause of UGI bleed, which included both variceal as well as nonvariceal causes.
Various studies from different parts of India have shown variable results. Studies from Southern and Eastern India showed PUD, whereas studies from Chandigarh showed variceal bleeds to be the most common cause of UGI bleed (7). However, they did not look into the cause of variceal bleed, whether it was cirrhosis or NCPH, and the causes of cirrhosis. We had an important observation that variceal bleed is due to cirrhosis. Moreover, fundal varices, which present with massive GI bleed, are more common in NCPH than cirrhosis of the liver. Rathi et al. reported that in 45.5% of the patients, UGIB was due to esophageal varices (3). It appears that due to improvement in hygiene, sanitation, and socioeconomic status, the prevalence of NCPH is on a declining trend. Also, due to better medical facilities and access to health care system, pediatric diarrheal diseases and umbilical sepsis have reduced considerably, which were significant risk factors for noncirrhotic portal hypertension (8). In Asia, chronic hepatitis B is the most common cause of chronic liver disease, (9) whereas Western studies have shown that alcoholic liver disease is more common (10). There is a changing trend in India, which has been observed in various studies, that instead of chronic viral hepatitis, alcoholic liver disease has superseded other causes of CLD. Furthermore, cryptogenic cirrhosis, which is mostly nonalcoholic steato-hepatitis (NASH)-related cirrhosis, was next to alcohol as a cause of chronic liver disease. Singh et al. recently reported that alcohol-related disease, not HBV, is the major cause of liver cirrhosis in Asia (11). We had also reported alcohol in 58–66% of patients, followed by NASH in 9–14% of patients, as a cause of cirrhosis (12–14). This is in accordance with Western data where NASH-related CLD is an upcoming epidemic and is becoming the leading cause of liver transplantation (15).
In the present study, we documented that unlike PUD in previous studies, esophagitis and erosive gastritis were the most common causes of nonvariceal bleeds. Careful history revealed that most of these patients were alcoholics. Over-the-counter use of proton pump inhibitors and their liberal use by all specialists have decreased the incidence of PUD and definitely reduced bleeds related to PUD. In our study, only 28 patients had bleed due to PUD, out of which 23 were noncirrhosis and 5 were cirrhosis patients.
In our study, 26% of the UGIB was due to nonvariceal causes. A study from Nepal reported nonvariceal causes of UGI bleed accounting for 33.3% of the cases (16). However, in their study, PUD was the most common cause (19.2% of total UGIB), while in our study, esophagitis accounted for 34.5% of the nonvariceal cause. In a study by Romcea et al., almost 27% of cirrhotic patients with UGI hemorrhage had bleeding from a nonvariceal source, the most common etiology being peptic ulcer (17). In the present study, no cause of UGIB could be documented in 32 (9%) of the patients possibly due to late presentation to our center and receiving medical treatment from referring hospitals. Most of these patients should be included under the nonvariceal group as erosions and ulcers tend to heal fast when treated medically with proton pump inhibitors. And, even if they have an UGIE done after 48 h, the lesions may have healed. It was also shown that there was a lesser number of bleeding episodes in cirrhosis with larger volume of bleed per episode and lower hemoglobin values on admission, suggesting that they are more seriously ill requiring more blood transfusions.
Overall, cirrhotic portal hypertension is becoming the most common cause of UGI bleed and alcohol is emerging as the commonest cause of UGI bleed including variceal and nonvariceal bleeds. As effective antiviral therapy is on the way of eliminating chronic viral hepatitis B and C, we have to acknowledge alcohol and NASH as emerging causes of CLD in India. UGI bleed is an important cause of mortality in the emergency department for patients awaiting emergency endoscopy. The changing trend in the causes of UGI bleed will guide us for more effective pharmacological and interventional therapies in this group of patients.
Conflict of Interest
Tarana Gupta and Sandeep Goyal declare they have no conflict of interest.
Financial Disclosure
Nil.
REFERENCES
1. Longstreth GF. Epidemiology of hospitalization for acute upper gastrointestinal hemorrhage: A population-based study. Am J Gastroenterol. 1995;90:206–10.
2. Silverstain FE, Gilbert DA, Tedesco FJ, Buenger NK, Persing J. The national ASGE survey on upper gastrointestinal bleeding. II Clinical prognostic factors. Gastrointestinal Endosc.1981;27:80–93. 10.1016/S0016-5107(81)73156-0
3. Rathi P, Abraham P, Jakareddy R, Pai N. Spectrum of upper gastrointestinal bleeding in Western India. Indian J Gastroenterol. 2001;20(Suppl 2):A37.
4. Gajendra O, Ponsek T, Varghese J, Sadasivan S, Nair P, Narayanan VA. Single center study of upper GI endoscopic findings in patients with overt and occult upper GI bleed. Indian J Gastroenterol. 2009;28:A111.
5. Anand CS, Tandon BN, Nundy S. The causes, management and outcome of upper gastrointestinal haemorrhage in an Indian hospital. Br J Surg. 1983;70:209–11. 10.1002/bjs.1800700407
6. Krishnakumar R, Padmanabhan P, Premkumar, Selvi C, Ramkumar, Joe A. Upper GI bleed–A study of 408 cases. Indian J Gastroenterol. 2007;26(Suppl 2):A133.
7. Sharma V, Jeyaraman P, Rana SS, Gupta R, Malhotra S, Bhalla A, et al. Utility of clinical and complete Rockall score in Indian patients with upper gastrointestinal bleeding. Trop Gastroenterol. 2016;37:276–82. 10.7869/tg.373
8. Sarin SK, Kumar A, Chawla YK, Baijal SS, Dhiman RK, Jafri W, et al. Noncirrhotic portal fibrosis/idiopathic portal hypertension: APASL recommendations for diagnosis and treatment. Hepatol Int. 2007;1(3):398–413. 10.1007/s12072-007-9010-9
9. Merican I, Guan R, Amarapuka D, Alexander MJ, Chutaputti A, Chien RN, et al. Chronic hepatitis B virus infection in Asian countries. J Gastroenterol Hepatol. 2000;15:1356–61. 10.1046/j.1440-1746.2000.0150121356.x
10. Liangpunsakul S, Haber P, McCaughan GW. Alcoholic liver disease in Asia, Europe, and North America. Gastroenterology. 2016;150:1786–97. 10.1053/j.gastro.2016.02.043
11. Singh SP, Panigrahi S, Mishra D, Khatua CR. Alcohol-associated liver disease, not hepatitis B, is the major cause of cirrhosis in Asia. J Hepatol. 2019;70:1031–2. 10.1016/j.jhep.2019.01.003
12. Agrawal S, Duseja A, Gupta T, Dhiman RK, Chawla Y. Simple organ failure count versus CANONIC grading system for predicting mortality in acute-on-chronic liver failure. J Gastroenterol Hepatol. 2015;30:575–81. 10.1111/jgh.12778
13. Dhiman RK, Agrawal S, Gupta T, Duseja A, Chawla Y. Chronic liver failure-sequential organ failure assessment is better than the Asia-Pacific Association for the Study of liver criteria for defining acute-on-chronic liver failure and predicting outcome. World J Gastroenterol. 2014;20:14934–41. 10.3748/wjg.v20.i40.14934
14. Gupta T, Dhiman RK, Rathi S, Agrawal S, Duseja A, Taneja S, et al. Impact of hepatic and extrahepatic insults on the outcome of acute-on-chronic liver failure. J Clin Exp Hepatol. 2017;7:9–15. 10.1016/j.jceh.2016.10.006
15. Wong RJ, Aguilar M, Cheung R, Perumpail RB, Harrison SA, Younossi ZM, et al. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology. 2015;148:547–55. 10.1053/j.gastro.2014.11.039
16. Bhattarai S, Dewan KR, Shrestha G, Patowary BS. Spectrum of upper gastrointestinal bleed in patients with cirrhosis of liver. JCMS Nepal. 2017;13:318–22. 10.3126/jcmsn.v13i3.17938
17. Romcea AA, Tanţău M, Seicean A, Pascu O. The etiology of upper gastrointestinal bleeding in cirrhotic patients. Clujul Med. 2013;86:21–3.